gautam machiraju fp
TRANSCRIPT
SERPINA1 Regulation in COPD Patients
G. MACHIRAJU, UNIVERSITY OF CALIFORNIA, BERKELEY
(Submitted 7 December 2015)
This paper seeks to discuss the design and model of a novel gene circuit for Chronic Obstructive Pulmonary Disease (COPD) therapy. Through biochemical, mathematical, and computational analysis, we can better understand the disease’s nature in tandem with our proposed gene circuit, and thereby use this information to extrapolate its behavior in the future as a potential therapy.
I. MOTIVATION
COPD is a disease characterized by inflammatory degradation of lung plasticity leading to severe shortness of breath. Smoking has historically been the predominant cause of COPD, but in the wake of urbanization and industrialization, air pollutants have become a major player on the etiological stage.
Currently, it is projected that over 408.8 million people worldwide have died as a result of this diseases, thereby making COPD the third leading cause of death in the world.[11] In southeast Asia alone, it is projected that COPD diagnoses will increase by 70% within the next few years.[11] Yet, due to lack of awareness, over 50% of the at-risk population go undiagnosed until patients enter late stage disease — at which reversible therapeutics become obsolete and mechanical respiratory aid becomes a need.[11]
II. THE GENETICS OF COPD
Through epidemiological studies, COPD has shown to possess both environmental and genetic risk factors. Although the genetics of COPD, as with many disease, is not completely certain, there exist promising gene candidates to help pin down COPD pathogenesis. Recent research[1] has shown that low gene expression of SERPINA1, and subsequently deficient production of a serine protease inhibitor known as Alpha-1 Antitrypsin (AAT)[4], leads to some of the major
debilitating symptoms of COPD including the loss of lung plasticity — namely, through the high expression of elastase, which facilitates elastin degradation.[6][8]
III. CURRENT THERAPIES & NEEDS ANALYSIS
Currently, all treatments for COPD are to alleviate symptoms and are not curative. Today, most patients receive steroid and anti-inflammatory medication or even employ oxygenation if suffering from later stage COPD.
The only approved gene therapy treatment involves the intramuscular injection of AAT[1] using nonviral gene transfer, gammaretrovirus, recombinant adenovirus, and recombinant adeno-associated virus vectors.[2] This treatment can be thought of as a “pulse” of AAT into the genetic system; it is usually effective in response to a specific event common to COPD patients known as an acute exacerbation — a sudden, worsening of symptoms including shortness of breath and surge in phlegm production, usually due to environmental pollutants or infection[12] — but fails to treat patients in a long-term manner. This, therefore, sheds light on the need for automated regulation of elastase.
IV. THIS STUDY’S DESIGN
In this study, the goal of the experimental design and analysis is to create a gene therapy to tackle the very chronic nature of COPD by regulating lung tissue deterioration. Specifically, the aim is to create safe, regulatory SERPINA1
2 Machiraju
expression in COPD patients to relieve them of their chronic symptoms. This can be achieved by introducing a genetic circuit that senses elastase and cellular markers, and regulates SERPINA1 expression correspondingly. The specific components needed for this circuit are: (1) sensors, (2) actuators, and (3) our delivery method. 1. Sensors
This study aims to create a sensor that will sense for the presence of elastase complex, as well as a cell type-specific biomarker which will then lead to the correspondingly regulation of SERPINA1.
Through lung biopsies of COPD patients, it has been observed that excess elastin degrades the walls of the alveoli (epithelial and squamous, and interstitial cells)[15][16]. Therefore, alveolar cell type biomarkers (e.g. purinergic receptor P2X 7 (P2X7) or gamma-aminobutyric acid receptor pi subunit (GABRP)[19]) make great potential candidates for this study.
The sensor for the elastase is a transcriptional promoter at which the rate of binding regulates transcription. On the other hand, the sensor for the cellular biomarker is a translation-inactivated mRNA aptamer, in which binding induces a conformational change and activates the mRNA to linearize and allow itself to become translated. 2. Actuators
The actuator for this study detects both elastase and our cellular biomarker, thereby forming a 2-input AND gate and spanning both the transcriptional and translational levels of gene expression.
If both inputs are present, the AND gate then expresses our selected model gene (G) — a potential candidate is HNF4A,[20] as its protein HNF4 shows promise in its interaction with SERPINA1’s promoter. The aim is to have the AND gate operate on
thresholds found via literature searches. Furthermore, the AND gate’s corresponding responses are either activating SERPINA1 production if both elastase and cellular biomarker are high, or correspondingly fail to activate SERPINA1 and allow for the repression of elastase.
3. Delivery Methods This then begs the question of how
to deliver this gene therapy. In this study’s design, the plan is to employ transient transfection — in other words, engineer the AND gate portion of the circuit within a plasmid and deploy it into the patient via bacteriophage injection.
With this delivery regime, alveolar cells can independently induce responses on themselves (either SERPINA1 activation or no SERPINA1 activation) based their own states (presence of elastase and the cell type biomarkers).
This study chose to implement eukaryotic transfection of a plasmid that senses elastase to allow for a more reliable delivery of elastase as a transcription factor — elastase can be transported within alveolar cells, but not as readily in other cell types. Additionally, the cell’s own biomarkers and SERPINA1 gene will be naturally found in our cells of interest, completing the search of necessary and viable inputs. This selection fulfills the need for alveolar cells to sense and actuate on themselves with inputs that can be found internally.
This circuit, as a whole, will thereby detect for abnormalities from within alveolar cells and then allow them to act via gene expression — with a return to steady and healthy levels of SERPINA1 expression and desired phenotypic recovery. This form of therapy seeks to be more effective than the current treatment, which only introduces additional AAT into the bloodstream via injection, therefore not allowing for
SERPINA1 Regulation in COPD Patients 3
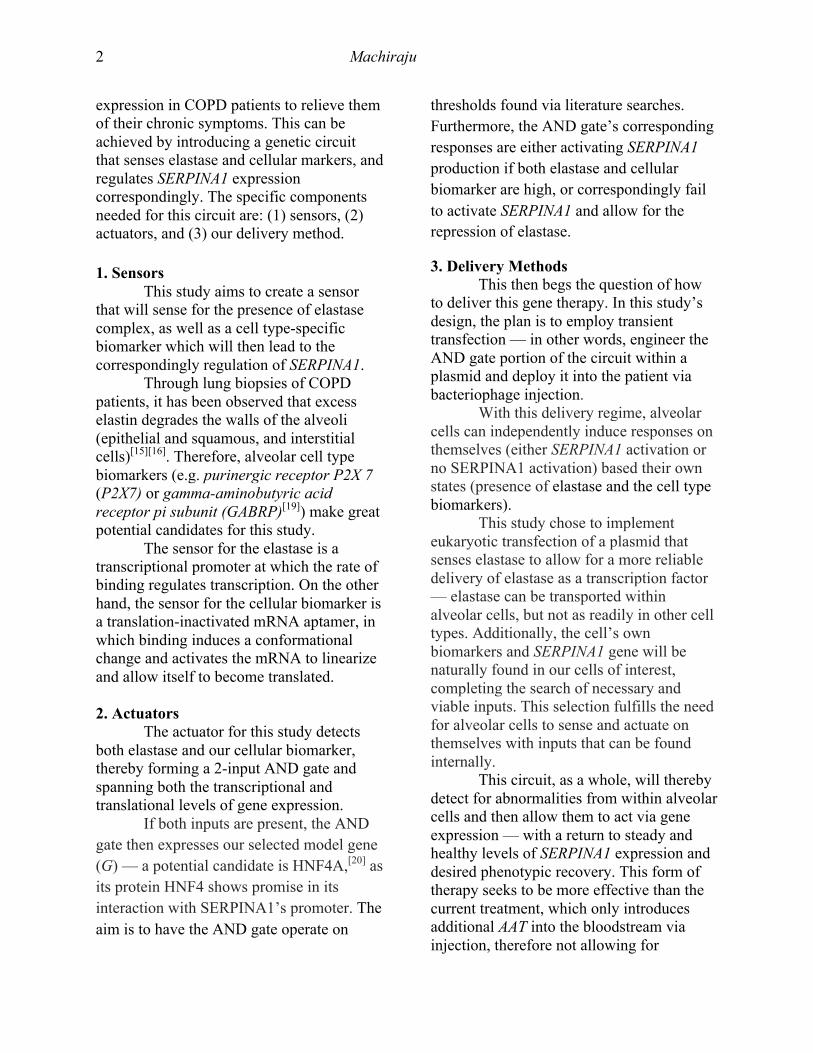
regulation within the biological system itself. Below is a detailed depiction of the proposed circuit (aptamer image adapted from [22]):
V. MATHEMATICAL ANALYSIS
This system can be constructed and analyzed as a system of differential equations, allowing us to review theoretical performance before further steps toward clinical implementation. In many cases, unaccounted biological noise and complexity, stability and instability regions, boundary and steady state conditions, and system thresholds, are identified in vitro, leading for re-evaluation prior to in vivo studies and clinical trial efforts. The following is a mathematical model of our system, which utilizes second order equations and the framework of transient transfection: 𝑑[𝑚𝑅𝑁𝐴!]
𝑑𝑡= 𝑘!"#[𝑃1 ∷ 𝐺𝑃] − 𝑘!"#$[𝑚𝑅𝑁𝐴!]
𝑑 𝑚𝑅𝑁𝐴!"𝑑𝑡 = 𝑘!"# 𝑃2 ∷ 𝐸 + 𝑘![𝑚𝑅𝑁𝐴!"] − 𝑘!"#$[𝑚𝑅𝑁𝐴!"]
𝑑 𝑚𝑅𝑁𝐴!"𝑑𝑡
= 𝑘! 𝑚𝑅𝑁𝐴!" [𝑐𝑚] − 𝑘!"!"[𝑚𝑅𝑁𝐴!"]
𝑑 𝑚𝑅𝑁𝐴!𝑑𝑡
= 𝑘!"#"$ − 𝑘!"#$[𝑚𝑅𝑁𝐴!]
𝑑[𝐴𝐴𝑇]𝑑𝑡
= 𝑘!"# 𝑚𝑅𝑁𝐴! − 𝑘!"# 𝐴𝐴𝑇 [𝐸] − 𝑘!"#$[𝐴𝐴𝑇]
𝑑[𝐺𝑃]𝑑𝑡
= 𝑘!"#[𝑚𝑅𝑁𝐴!"] − 𝑘!"#$[𝐺𝑃]
𝑑[𝐸]𝑑𝑡
= 𝑘!"# 𝑚𝑅𝑁𝐴! − 𝑘!"# 𝐴𝐴𝑇 𝐸 − 𝑘!"#$[𝐸]
𝑑[𝑃2]𝑑𝑡 = 𝑘!"!#$% − 𝑘!"#$% 𝑃2 + 𝑃2 ∷ 𝐸 − 𝑘!"![𝑃2][𝐸]
− 𝑘!""![𝑃2 ∷ 𝐸]
𝑑[𝑃1]𝑑𝑡 = 𝑘!"!#$% − 𝑘!"#$% 𝑃1 + 𝑃1 ∷ 𝐺𝑃 − 𝑘!"![𝑃1][𝐺𝑃]
− 𝑘!""![𝑃1 ∷ 𝐺𝑃]
𝑑 𝑃2 ∷ 𝐸𝑑𝑡
= 𝑘!"! 𝑃2 [𝐸] − 𝑘!""![𝑃2 ∷ 𝐸]
𝑑 𝑃1 ∷ 𝐺𝑃𝑑𝑡
= 𝑘!!! 𝑃1 [𝐺𝑃] − 𝑘!""![𝑃1 ∷ 𝐺𝑃]
This model decided against using Hill functions to represent promoter binding largely because of the values being bounded by [0,1] — this fact doesn’t allow for the representation of promoter concentrations, which are very important for transient transfection regimes. Referring to the model depiction, below is a key to identify which species are undergoing dynamics:
mRNAS – mRNA encoding SERPINA1 AAT – naturally occurring elastase inhibitor; SERPINA1’s translated protein mRNAE – mRNA encoding ELANE gene; produced at basal level E – elastase protein mRNAGi – inactivated mRNA encoding G mRNAGa – activated mRNA encoding G GP – G’s translated protein P1 – SERPINA1’s promoter P2 – G’s promoter cm – cellular biomarker :: – indicates binding ktxn, ktln –transcription and translation rates ka, ki – activation and inactivation rates for mRNAG aptamer kbasal – basal expression of mRNAE kmdeg – mRNA degradation rate kpdeg – protein degradation rate kplprod, kpldeg – production and degradation rates
for transfected plasmid kon1, kon2 – promoter binding rates koff1, koff2 – promoter unbinding rates
4 Machiraju
VI. ASSUMPTIONS
Assumptions include kpdeg is a shared rate among all protein degradation reactions and kmdeg is a shared rate among all mRNA degradation reactions. It should also be noted that the kpdeg, kmdeg, and kpldeg constants multiplied to concentrations represent degradation terms and the complementary positive products represent production terms.
It is also assumed that our promoter dynamics are all coupled together with the dynamics of plasmid degradation and production in our transient transfection model. In other words, promoter production is dependent on plasmid propagation while promoter degradation is dependent on the cell cycle. Below is a representation of this interaction, where P is any promoter and TF is any transcription factor:
Another assumption lies in the interaction between AAT and elastase; this study assumes a sequestration reaction in which AAT renders elastase non-functional by binding to its active site. Furthermore, although thermodynamic principles require that there are forward and reverse reactions for the binding of this small molecule to its repressor, the reverse reaction is assumed to be so slow that we claim that it is negligible — thereby giving us an irreversible sequestration reaction scheme below:
Additionally, this model makes no assumption that mRNA dynamics are much faster than protein dynamics and can be ignored — this is done in order to make it more realistic.
It should also be noted that many of the rate parameters and constants in this model were arbitrarily decided on, but are comparable to values found in similar reactions. This is due to the fact that many of this reaction’s experimental rate constants are not yet determined. The units of this model were determined via transient transfection metrics: the cell cycle of alveolar cells has been experimentally determined to be 120 days, [21] thereby giving us
𝑘𝑝𝑙𝑑𝑒𝑔 =ln (2)24 ∗ 120
and hours-1 as our units of rate constants.
VII. COMPUTATIONAL ANALYSIS & RESULTS
For the most of the analysis, this study utilized the MATLAB simBiology software toolkit to glean insight into the general dynamics of the proposed model, points of stability, and a parameter scanning and sensitivity analysis. The results will be performed numerically and continuously and will yield temporal models.
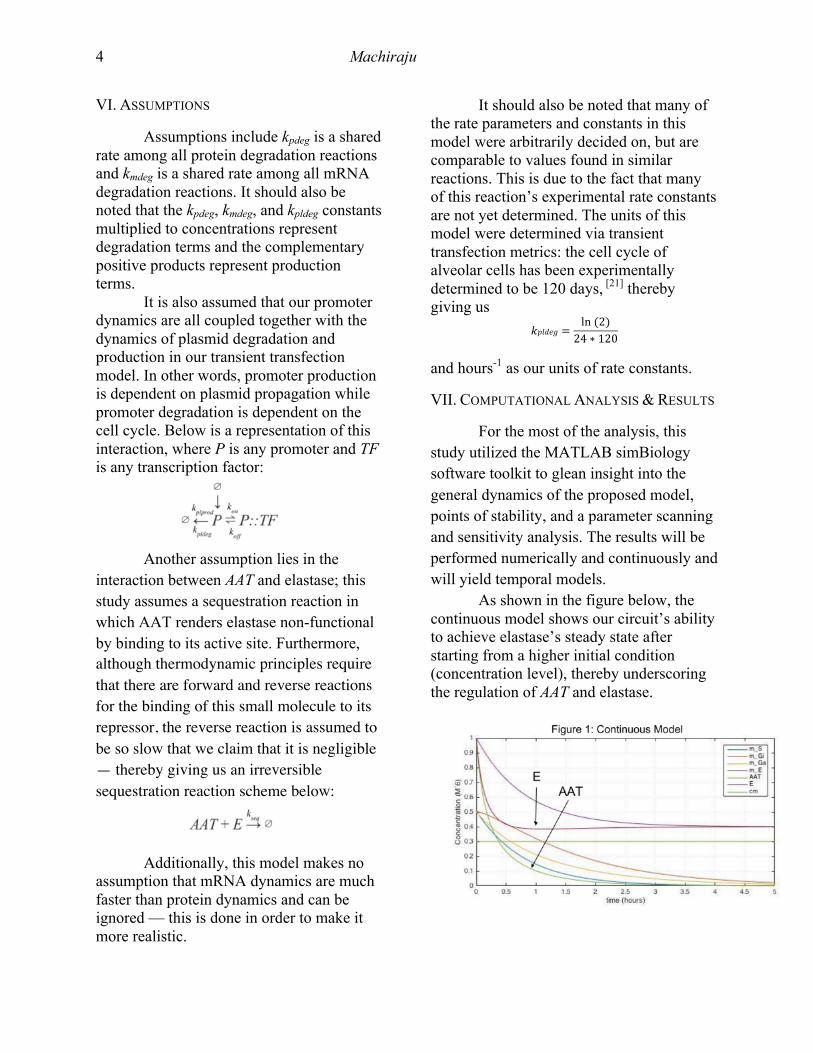
As shown in the figure below, the continuous model shows our circuit’s ability to achieve elastase’s steady state after starting from a higher initial condition (concentration level), thereby underscoring the regulation of AAT and elastase.
SERPINA1 Regulation in COPD Patients 5
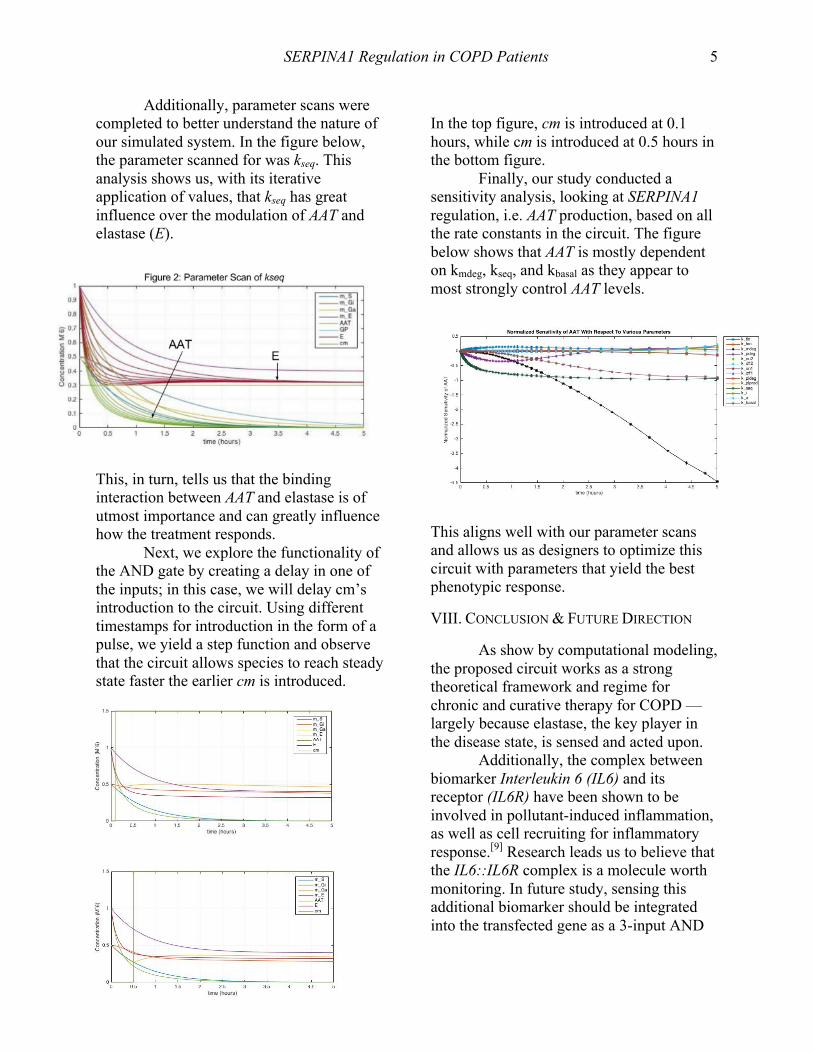
Additionally, parameter scans were completed to better understand the nature of our simulated system. In the figure below, the parameter scanned for was kseq. This analysis shows us, with its iterative application of values, that kseq has great influence over the modulation of AAT and elastase (E).
This, in turn, tells us that the binding interaction between AAT and elastase is of utmost importance and can greatly influence how the treatment responds.
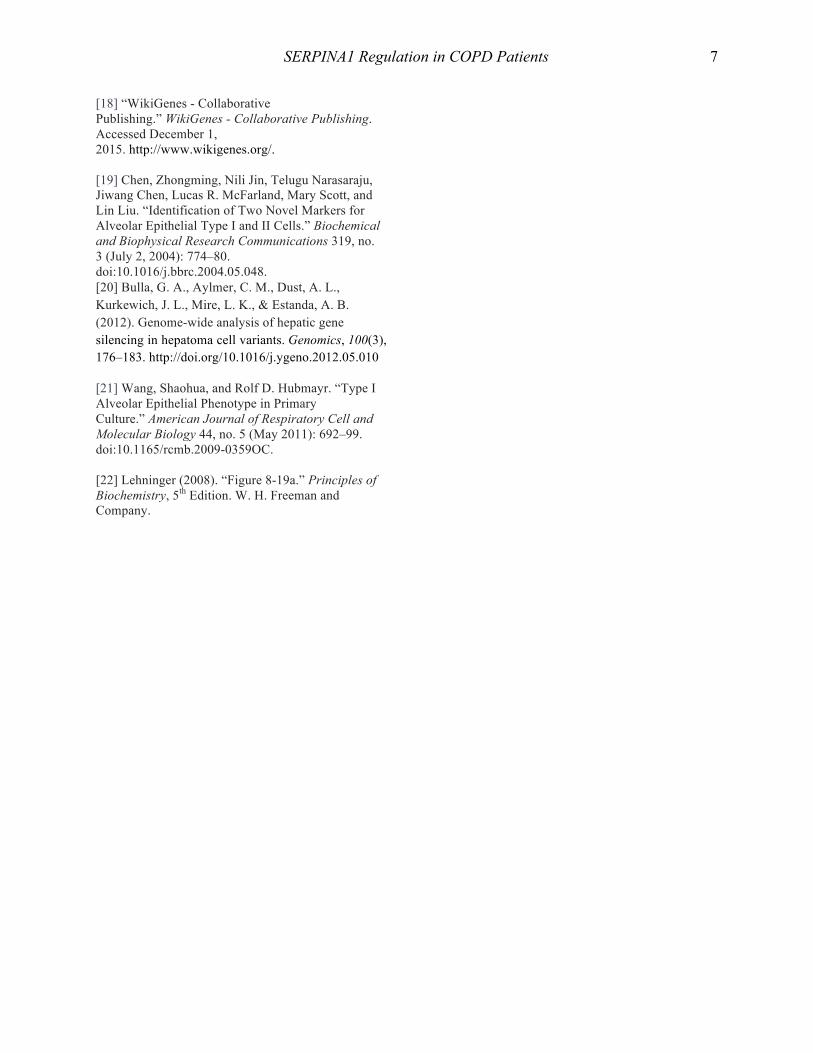
Next, we explore the functionality of the AND gate by creating a delay in one of the inputs; in this case, we will delay cm’s introduction to the circuit. Using different timestamps for introduction in the form of a pulse, we yield a step function and observe that the circuit allows species to reach steady state faster the earlier cm is introduced.
In the top figure, cm is introduced at 0.1 hours, while cm is introduced at 0.5 hours in the bottom figure.
Finally, our study conducted a sensitivity analysis, looking at SERPINA1 regulation, i.e. AAT production, based on all the rate constants in the circuit. The figure below shows that AAT is mostly dependent on kmdeg, kseq, and kbasal as they appear to most strongly control AAT levels.
This aligns well with our parameter scans and allows us as designers to optimize this circuit with parameters that yield the best phenotypic response.
VIII. CONCLUSION & FUTURE DIRECTION
As show by computational modeling, the proposed circuit works as a strong theoretical framework and regime for chronic and curative therapy for COPD — largely because elastase, the key player in the disease state, is sensed and acted upon.
Additionally, the complex between biomarker Interleukin 6 (IL6) and its receptor (IL6R) have been shown to be involved in pollutant-induced inflammation, as well as cell recruiting for inflammatory response.[9] Research leads us to believe that the IL6::IL6R complex is a molecule worth monitoring. In future study, sensing this additional biomarker should be integrated into the transfected gene as a 3-input AND

6 Machiraju
gate on the transcriptional level to add even greater specificity to our system.
Despite having a cell-type biomarker as a check to add specificity to our system, a potential drawback for this design is that the transfected plasmid would propagate within all cells and not just our desired cell type. Future study would also determine and implement a mechanism to restrict bacteriophage plasmid deployment to specific cell types (e.g. surface protein detection) in order to remedy this issue.
IX. REFERENCES
[1] Al-Jamal, R., W. a. H. Wallace, and D. J. Harrison. “Gene Therapy for Chronic Obstructive Pulmonary Disease: Twilight or Triumph?”Expert Opinion on Biological Therapy 5, no. 3 (March 2005): 333–46. doi:10.1517/14712598.5.3.333. [2] Mueller, Christian, and Terence R. Flotte. “Gene-Based Therapy for Alpha-1 Antitrypsin Deficiency.” COPD 10 Suppl 1 (March 2013): 44–49. doi:10.3109/15412555.2013.764978. [3] “SERPINA1 Gene Pathway.” Accessed December 1, 2015. https://targetexplorer.ingenuity.com/gene/EG/5265/interaction#!/api/rest/v1/client/searchPathwayNodes?pathwayId=ING:1nilf&rows=0&facetLimit=5000&responseType=default. [4] “Alpha-1 Antitrypsin.” Wikipedia, the Free Encyclopedia, November 19, 2015. https://en.wikipedia.org/w/index.php?title=Alpha-1_antitrypsin&oldid=691416498. [5] Akira, S., H. Isshiki, T. Sugita, O. Tanabe, S. Kinoshita, Y. Nishio, T. Nakajima, T. Hirano, and T. Kishimoto. “A Nuclear Factor for IL-6 Expression (NF-IL6) Is a Member of a C/EBP Family.” The EMBO Journal 9, no. 6 (June 1990): 1897–1906. [6] “SERPINA1 Serpin Peptidase Inhibitor, Clade A (alpha-1 Antiproteinase, Antitrypsin), Member 1 [Homo Sapiens (human)] - Gene - NCBI.” Accessed December 8, 2015. http://www.ncbi.nlm.nih.gov/gene/5265. [7] “KLKB1 Kallikrein B1 [Homo Sapiens (human)] - Gene - NCBI.” Accessed December 8, 2015. http://www.ncbi.nlm.nih.gov/gene/3818.
[8] “Elastase.” Wikipedia, the Free Encyclopedia, May 26, 2015. https://en.wikipedia.org/w/index.php?title=Elastase&oldid=664077037. [9] Berndt, Annerose, Adriana S Leme, and Steven D Shapiro. “Emerging Genetics of COPD.” EMBO Molecular Medicine 4, no. 11 (November 2012): 1144–55. doi:10.1002/emmm.201100627. [10] Kloth, J. N., A. Gorter, G. J. Fleuren, J. Oosting, S. Uljee, N. ter Haar, E. J. Dreef, G. G. Kenter, and E. S. Jordanova. “Elevated Expression of SerpinA1 and SerpinA3 in HLA-Positive Cervical Carcinoma.” The Journal of Pathology 215, no. 3 (July 2008): 222–30. doi:10.1002/path.2347. [11] “WHO | World Health Organization.” WHO. Accessed December 8, 2015. http://www.who.int/en/. [12] “Acute Exacerbation of Chronic Obstructive Pulmonary Disease.” Wikipedia, the Free Encyclopedia, October 13, 2015.https://en.wikipedia.org/w/index.php?title=Acute_exacerbation_of_chronic_obstructive_pulmonary_disease&oldid=685525919. [13] Thorley, Andrew J, and Teresa D Tetley. “Pulmonary Epithelium, Cigarette Smoke, and Chronic Obstructive Pulmonary Disease.”International Journal of Chronic Obstructive Pulmonary Disease 2, no. 4 (December 2007): 409–28. [14] O’Donnell, R, D Breen, S Wilson, and R Djukanovic. “Inflammatory Cells in the Airways in COPD.” Thorax 61, no. 5 (May 2006): 448–54. doi:10.1136/thx.2004.024463. [15] “Pulmonary Alveolus.” Wikipedia, the Free Encyclopedia, November 22, 2015. https://en.wikipedia.org/w/index.php?title=Pulmonary_alveolus&oldid=691828277. [16] “Alveolar Cells.” Wikipedia, the Free Encyclopedia, November 10, 2015. https://en.wikipedia.org/w/index.php?title=Alveolar_cells&oldid=689941179. [17] “Lung Microbiome.” Wikipedia, the Free Encyclopedia, November 3, 2015. https://en.wikipedia.org/w/index.php?title=Lung_microbiome&oldid=688801668.
SERPINA1 Regulation in COPD Patients 7
[18] “WikiGenes - Collaborative Publishing.” WikiGenes - Collaborative Publishing. Accessed December 1, 2015. http://www.wikigenes.org/. [19] Chen, Zhongming, Nili Jin, Telugu Narasaraju, Jiwang Chen, Lucas R. McFarland, Mary Scott, and Lin Liu. “Identification of Two Novel Markers for Alveolar Epithelial Type I and II Cells.” Biochemical and Biophysical Research Communications 319, no. 3 (July 2, 2004): 774–80. doi:10.1016/j.bbrc.2004.05.048. [20] Bulla, G. A., Aylmer, C. M., Dust, A. L., Kurkewich, J. L., Mire, L. K., & Estanda, A. B. (2012). Genome-wide analysis of hepatic gene silencing in hepatoma cell variants. Genomics, 100(3), 176–183. http://doi.org/10.1016/j.ygeno.2012.05.010
[21] Wang, Shaohua, and Rolf D. Hubmayr. “Type I Alveolar Epithelial Phenotype in Primary Culture.” American Journal of Respiratory Cell and Molecular Biology 44, no. 5 (May 2011): 692–99. doi:10.1165/rcmb.2009-0359OC. [22] Lehninger (2008). “Figure 8-19a.” Principles of Biochemistry, 5th Edition. W. H. Freeman and Company.