print issn 0972-0200 e-issn 0976-2892 delhi journal of ... · new delhi new delhi noida daryaganj,...
TRANSCRIPT
1www.djo.org.in
E-ISSN 0976-2892
Print ISSN 0972-0200 E-ISSN 0976-2892DELHI JOURNAL OF OPHTHALMOLOGY
JOURNAL OF DELHI OPHTHALMOLOGICAL SOCIETY
EDITOR IN CHIEF
M. VanathiDr R P Centre, AIIMS, New Delhi
EXECUTIVE EDITORS Zia Chaudhuri Harinder Singh Sethi Uma Sridhar Manisha Agarwal LHMC & Dr R ML Hospitals Safdarjung Hospital Icare Hospital Dr Shroff’s Charity Eye Hospital New Delhi New Delhi Noida Daryaganj, Delhi EDITORIAL BOARD Umang Mathur Rachna Meel Sima Das Neelam Pushker Viney Gupta Cornea, Cataract & Refractive Ophthalmoplasty, Ophthalmoplasty, Ophthalmoplasty, Glaucoma, Dr Shroff’s Charity Eye Hospital, Dr RML Hospital, Dr Shroff’s Charity Eye Dr R P Centre, AIIMS Dr R P Centre, AIIMS New Delhi New Delhi Hospital, New Delhi New Delhi New Delhi Gaurav Kakkar Saurabh Sawhney Raminder Bakshi Charu Khurana Geetha Srinivasan Pediatric Ophthalmology, Cataract & Refractive, Cornea & Refractive, Refractive Surgery Strabismus, Icare Venu Eye hospital, New Delhi Insight Eye Clinic, New Delhi CFS, New Delhi CFS, New Delhi Hospital,Noida Ramesh Venketesh Parijat Chandra Shalini Mohan Anshu Arora Reena Sharma Retina, Dr Shroff’s Charity Retina, Dr R P Centre Kanpur Medical Retina, Strabismus, Dr R P Centre, Eye Hospital, New Delhi AIIMS, New Delhi College, Kanpur Icare Hospital, Noida AIIMS, New Delhi
EDITORS EMERITUS Dinesh Talwar V P Gupta Arun Sangal Mahipal S Sachdev Kamlesh Ajay Arora Rajpal Rohit Saxena Rajesh Sinha
ASSISTANT EDITORS Dewang Angmo Vishnukant Srilathaa G Digvijay Singh Bharat Patil Ravi Bypareddy Dr R P Centre, AIIMS Dr R P Centre, AIIMS Dr R P Centre, AIIMS Dr R P Centre, AIIMS Dr R P Centre, AIIMS Dr R P Centre, AIIMS New Delhi New Delhi New Delhi New Delhi New Delhi New Delhi
EDITORIAL ASSISTANTS Reetika Sharma Pinto Gautam Lokdarshi Rahul Mayor Anita Ganger Amrita Sawhney Metu Rajput Manish Mahabir Vineet Sehgal
EDITORIAL FORMATTING & ASSISTANCEVarun Kumar
DELHI ADVISORY BOARD Rajvardhan Azad Anita Panda J S Titiyal Rajinder Khanna P V Chadha B P Gulliani Amit Khosla Lalit Verma Harbans Lal Vimla Menon Atul Kumar Yograj Sharma J K S Parihar A K Grover S Khokhar Shashi Vashist M C Agarwal Ritu Arora Upreet Dhaliwal Anup Goswami Jolly Rohtagi Vishnu Gupta Namrata Sharma Ramanjit Sihota Tanuj Dada Narottama Sindhu M D Singh Madan Mohan Taru Dewan Abhishek Dagar RajeshJain KirtiSingh YogeshGuptaHarishGandhi PKSahu CyrusShroff Gopal K Das Rajesh Hans Pravin Malik Radhika Tandon Sangeetha Abrol B Ghosh Kamna Verma Sumit Kandhuja Anita Sethi R B Jain
NATIONAL ADVISORY BOARD R D Ravindran S Natarajan Barun K Nayak Samar Basak Jyotirmay Biswas D. Ramamurthi Abhay Vasavada Virendra Sangwan Arulmozhivarman Santosh Honavar Nirmal Fredrick D Bhattacharya Sajjad Ahmed Sheikh Arup Chakraborti M S Ravindra Rohit Shetty Sujatha Mohan S K Pandey A Bhattacharya Chandana Chakraborty Partha Biswas Venkatesh Prajna Rupal Shah Mukesh Taneja Sri Ganesh Mahesh Shanmugam Cyres Mehta Amar Agarwal Amod Gupta
Editorial Board
2 Del J Ophthalmol 2013;24(1)
ISSN 0972-0200
Delhi Journal of Ophthalmology
The JournalDelhi Journal of Ophthalmology (DJO) (ISSN Print: 0971-0200, Online: 0976-2892) is a peer reviewed journal published on behalf of Delhi Ophthalmological Society (DOS). The Journal publishes information relating to Ophthalmology, Vision Sciences and Ophthalmic Research. The journal is published in January – March, April – June, July – September, October – December.
Information for authors
Payment Information
This journal is indexed with Indian Science Abstracts and is currently under consideration for indexing with Index Copernicus
There are no page charges for manuscripts accepted for publication in DJO. Please check the journal website http://www.djo.org.in for online submission details. All manuscripts must be submitted online.
DJO is distributed free to all members of DOS. A subscription to DJO comprises of 4 issues, inclusive of postage charges. Annual Subscription for non-members includes:Institutional = INR Rs 4500 for IndiaUSD 160 for outside IndiaIndividual = INR Rs 3500 for IndiaUSD 100 for outside IndiaFor payment details please write to [email protected] / [email protected]
Claims for missing issues will be serviced at no charges if received within 60 days of the date of publication for domestic subscribers. Duplicate copies will not be sent in the event of failure of delivery due to non-communication of change in address. The journal is published and distributed by DOS from the DOS Secretariat. DJO is distributed for private communication to DOS members and copies obtained otherwise are illegal and cannot be resold or given away for commercial or library use. The copies of DJO will be couriered to all DOS members. The editorial board, association or publisher will not be responsible for non-receipt of issues. Members / Institution who wish to obtain DJO through registered post may kindly contact the DJO office. In the event of a copy of DJO returning due to change of address, incomplete/inaccurate address of a DOS member or subscriber on two or more occasions, the names of such members will be removed from the journal’s mailing list. Provision of complete contact details and mailing addresses is the responsibility of the member / subscriber.
Change of address information is to be sent to the editors office through post / or by email to [email protected].
The contents of DJO are protected by Indian and international copyrights. DJO grants free access of its printed text and permission to make copies of print material, to all users and permits use of its material in any digital medium for any reasonable non-commercial use with due acknowledgement of authorship and ownership of rights
The journal accepts display and classified advertising. Frequency discounts and special positions are available. Advertisements enquiries are to be addressed to [email protected] Journal reserves the right to reject any advertisement considered unsuitable according to the set policies of the journal. Advertisements printed in DJO do not attribute to any form of endorsement of the product by the journal or approval of the quality / value or claims staked by the advertising personnel.
General Information
Abstracting and Indexing information
Advertising policies
Copyright
General Information
Request for permissions to reproduce articles / information printed in DJO should be sent by post and / or email directed to the Editor-in-chief, DJO.
Permissions

3www.djo.org.in
E-ISSN 0976-2892
The opinions expressed in DJO and information published in it is not that of DJO or its Editorial Board members or the publisher. Publication is not indicative of endorsement of the journal. Neither DJO nor its publishers nor anyone else involved in the process of writing, editing, publishing or delivering the journal entail to the responsibility or liability of the accuracy of any information provided in DJO nor shall they be liable to any damage ( direct, indirect, special, incidental consequential or punitive) arising out of the use of DJO. DJO, nor its publishers nor anyone involved in the production of the material printed in the journal do not warrant to the accuracy of information published or are not responsible for any errors or omissions of the material published or for results ensuing from such material. Readers are encouraged to confirm the accuracy of information contained in the publication.The journal or the society will not be responsible for the views projected in the manuscripts. Views/ information expressed in articles published by DJO are the sole responsibility of the authors.
Disclaimer
Contact Address
Published by Delhi Ophthalmological Society Editorial Office:Dr M.Vanathi MD
Editor–in-Chief Delhi Journal of Ophthalmology
DOS Secretariat, Room No 479, 4th floorDr R P Centre For Ophthalmic Sciences
AIIMS, New Delhi 110029Ph: 65705229, 26588074
Email: [email protected], [email protected]
Website: www.djo.org.in
General Information
Cover Page Design By: Dr Saurabh Sawhney
4 Del J Ophthalmol 2013;24(1)4
Delhi Journal of Ophthalmology
DJO Vol. 24 No. 1: July - September 2013
6. From the Editor’s Desk: Publish and CherishM.Vanathi
7. Phakic Intraocular Lenses: An Overview Sana Ilyas Tinwala, J S Titiyal
16. Intra-Stromal Corneal Ring Segments Ramendra Bakshi, Charu Khurana, Ritika Sachdev, Mahipal Sachdev
23. Efficacy of Corneal Collagen Crosslinking with Riboflavin and Ultraviolet A in Progressive Keratoconus Aneeta Jabbar, Seema KM
28. Comparison of Visual Evoked Potential Components In Female Patients of Primary Open Angle Glaucoma with Age Matched Control Females Ruchi Kothari, Pradeep Bokariya, Smita Singh, Ramji Singh
41. No-Assistant Technique: Simplified Haptic Externalization For Glued IOL Priya Narang
34. Ocular Dirofilaria repens: not rare Usha Kim, Mohit Gupta, N.Vidhya, Shanti
37. Ocular Cicatricial Pemphigoid: Case Report Revathi Rajaraman, Vaidee Vikram, Anita Raghavan
Editorial
Major Review
Original Article
Case Report
Techniques
Video on DJO Web Page www.djo.org.in
Cont
ents

68. Comparison of Ultrasound Biomicroscopy and Gonioscopy Features of Angle In Pre & Post Laser Peripheral Iridotomy Patients of Primary Angle Closure Glaucoma Shalini Mohan, Ramesh Chandra Gupta, Perwaz Khan, Rajnath Singh Kushwaha, Surendra kumar Sachan
69. Author’s reply Vaishali AP, Viral R, Mariam NM, Purvi B, Prajapati K, Nirav M
5www.djo.org.in
Delhi Journal of Ophthalmology
DJO Vol. 24 No. 1: July - September 2013
43. Limbal Epithelial Stem Cells in Corneal Regeneration Shweta Sharma, M.Vanathi, Sujata Mohanty, Radhika Tandon
51. Scleral Contact Lenses Nidhi Gupta, Minal Kaur, Abhilek
58. Posterior Scleritis Chandana Chakraborti, Krittka Pal Chowdhury
61. Vogt Koyanagi Harada Syndrome Pratik K.Shah, Bhavin J.Patel, Khushnood M.Sheikh, Manisha B.Shahstri
67. Echographic Evaluation of Retinoblastoma and Its Management Modalities Sima Das
63. Spontaneous Closure of Traumatic Macular Hole Khushboo Doctor, Uday Gajiwala, Rohan Chariwala, Kamini Patel
65. Waardenburg Syndrome Type II Joginder Pal Chugh, Prachi Jain, Rajender Singh Chauhan, Ashok Rathi
Recent Advances
Allied Ophthalmic Sciences
Photo Essay
Brief Communication
Letter to editor
Cont
ents

“Literature is my Utopia” Helen Keller
From the Editor’s DeskPUBLISH and CHERISH
Learning never ceases. It is an embodiment of keen intent to excel. Through the years of evolvement from a resident to a consultant, marked with incessant attempts to master the clinical science of ophthalmology, I realized that “much of what we have learnt is but a fistful and what we have to learn is as vast as the ocean”.
As a resident when I glossed through the pages of academic literature, the tweak of fear ruled, for the call was always “PUBLISH or PERISH”. What was the secret that needed to be unraveled to remove this fear? What is that which will make writing a joy to behold?
Young minds need to learn to evolve from just being good clinicians; they need to realize that in the world of academics, clinical performance gets noticed with the theatrics of honest writing that will help get the message across, compel the audience to notice and make the difference show.
Residents need to learn to perform ophthalmology, understand concepts, structure a hypothesis, embark on a methodology to prove it, maintain ethics during the path, derive the results through structured statistics and conclude with evidence and conviction. That is not the end, but rather the beginning, for that is when the thinking mind gets the pen rolling to get the essence of flavor of one’s ethical research or clinical experience across to the assembly.Scientific Writing is an art to be learnt, cultivated and mastered. Writing with intent to get noticed never works. Good writing always gets noticed. This is one world, where the boundaries do not exist. This is the world of academic knowledge, where giving never results in impoverishment. This is one world where commitment and diligence shows the difference.
Why PUBLISH?
Productivity is the best sign of your growth
Understanding that evolves to prove your point of contention
Benefit from what you have learnt and disseminate it to the society
Learning to get your message across effectively with evidence based approach
Integrate with integrity the results of your research
Savour the strength and satisfaction of the success of your work
Honour which comes along with every published academic work being read and appreciated
With these in mind, let us move into the next tenure of Delhi Journal of Ophthalmology. Delhi Journal of Ophthalmology now comes to you with a new international outlook and flavor.We, at the editorial office, will constantly strive to let this official scientific journal of DELHI OPHTHALMOLOGICAL SOCIETY shine beyond what it has achieved in the yester years, to heighten its standards to higher levels. We look forward to meaningful and high quality manuscripts to fill our portals of submission in the forthcoming months, to keep our review panel working at its optimal best.
From this edition, come new sections that have been structured to appeal to residents and clinicians, to enhance their zeal and fervor to read and contribute. The Techniques in Ophthalmology section now features a video as well, which can be viewed online on the website of Delhi Journal of Ophthalmology. Experts’ Deliberations paves way for interesting reading about a clinical scenario. Young Ophthalmologists can compete with the publication of their thesis work as original articles.
LO! BEHOLD THE PLEASURES OF THE REJUVENATED DELHI JOURNAL OF OPHTHALMOLOGY!
Editorial......
M.Vanathi, MD(Editor-in-chief, Delhi Journal of Ophthalmology)
I realize that this page today is a reality because of the labor of all of our Editors’ Emeritus. They have made it possible to look for goals beyond… I am, but just another conduit endeavoring to take it forward further…Please join hands in our efforts towards leading our journal to elevated heights. Your participation as a reader, contributor, reviewer and patron will go a long way in helping to reach our goal.
Writing has never been more joyous and blissful……….. Come forth, PUBLISH and CHERISH…
DOI: http://dx.doi.org/10.7869/djo.2013.1
7www.djo.org.in
E-ISSN 0976-2892
Phakic Intraocular LensesAn OverviewDelhi J Ophthalmol 2013; 24 (1): 7-15
Currently, there are four general approaches to correct refractive errors: refractive corneal surgery, crystalline lens surgery, and implantation of an intraocular lens (IOL) in the anterior or posterior chamber. In any case, the main goal of refractive surgery is the smallest residual refractive error preserving vision quality with the same visual capacity. In this review, the current status of phakic intraocular lens (pIOL) surgery to correct refractive errors is reviewed. Phakic IOL includes any lens located between the cornea and the anterior surface of the crystalline lens, which is left undisturbed inside the eye. The insertion of an implant in a phakic eye must be simple, precise, and reproducible and must produce successful optical results. In addition, implantation of a phakic IOL allows retention of accomodation and is reversible. Current IOL choice includes angle-fixated anterior chamber IOLs, iris-fixated anterior chamber IOLs, and the posterior chamber phakic IOL
Laser corneal refractive surgery has been used to correct a wide range of refractive errors and has proven to be effective and safe in most cases. Despite the use of highly optimized and customized laser treatments such as wave front-guided, aspheric, and topography-guided ablations, the physical limitations of corneal thickness, curvature, and tissue remodeling limit the indications for a safe corneal refractive procedure. Moreover, the optical quality of the outcomes may not be as good as desired, especially when treating high refractive errors.
When keratorefractive surgery is not the appropriate approach, either phakic intraocular lens (pIOL) implantation or refractive lens exchange (RLE) with IOL implantation should be considered. One of the main concerns about RLE in highly myopic eyes is the increased risk for retinal detachment (RD), especially in younger patients and in eyes with long axial lengths (>26 mm). The incidence of RD after RLE ranges from 0% to 8%.1,2
RLE causes loss of accommodation and should be avoided when the natural lens is still functional. In the absence of contraindications, pIOL implantation is the best approach in young patients with moderate to high refractive errors and in those who have a contraindication to a corneal refractive procedure (eg, thin corneas). Advantages are that pIOL implantation maintains accommodation and is reversible.
TypesPhakic IOLs comprise 3 types:
angle-supported anterior chamber, iris-claw anterior chamber, and posterior chamber. Each design has its own features, selection criteria, surgical technique, results, and complications. (Table 1) summarizes the main features of those that are U.S. Food and Drug Administration (FDA) approved or has CE marking.
Angle Supported Anterior Chamber phakic IOLs
In 1953, Strampelli3 implanted the first minus power anterior chamber IOL in phakic eyes to correct myopia. In 1959, Barraquer4 reported the results of 239 implantations. Although the first results were encouraging, many pIOLs had to be explanted owing to complications such as chronic loss of corneal endothelial cells, iris retraction and atrophy, peripheral anterior synechiae, subsequent pupil ovalization, and uveitis–glaucoma–hyphema syndrome.5,6
Current ModelsPolymethyl methacrylate Angle-Supported Anterior Chamber pIOLs: With the advent of foldable models, PMMA angle-supported pIOLs have been almost abandoned.
Keywords : myopia • hyperopia • refractive surgery • phakic IOL
Major Review
*Sana Ilyas Tinwala, J S TitiyalCornea & Ocular Surface, Cataract & Refractive Services,
Dr. Rajendra Prasad Centre, AIIMS,New Delhi - 110029, India
Sana Ilyas Tinwala MD
Dr. Rajendra Prasad Centre, AIIMS,New Delhi - 110029email id: [email protected]
*Address for correspondence
DOI: http://dx.doi.org/10.7869/djo.2013.2
8 Del J Ophthalmol 2013;24(1)
ISSN 0972-0200
Tinwala, Titiyal.
Foldable Angle Supported Anterior Chamber pIOLs: T h e s e pIOLs can be inserted through a 3.0 mm or smaller incision. Foldable IOLs and their haptics must be stiff enough to provide stability in the anterior chamber.
The Kelman Duet and the AcrySof IOLs have obtained the CE mark and are commercially available in Europe. The ThinPhAc and the Vision Membrane are in clinical trials in Europe and Russia.
w Kelman Duet: The Kelman Duet (Tekia, Inc.) consists of an independent Kelman tripod PMMA haptic with an overall diameter of 12.5, 13.0, or 13.5mm and a 5.5mm silicone optic with a ultraviolet (UV) absorber and a dioptric range of -8.0 to -20.0 D. The haptic is implanted first in the anterior chamber through an incision smaller than 2.5 mm; the optic is then inserted using an injector system; finally, the optic is fixated in the anterior chamber by the optic eyelets and haptic tabs using a Sinskey hook. If a calculation error in pIOL power or a refractive change occurs with time, the optic can be exchanged and assembled in the anterior chamber. If a haptic sizing error occurs, the haptics can be exchanged independently. The reported endothelial cell loss at 12 months is 5.43%,7 but mid-term and long-term complication rates are not yet available.
w AcrySof: The AcrySof (Alcon, Inc.) is a single piece, hydrophobic acrylic angle-supported pIOL manufactured as a 6.0 mm diameter meniscus optic with an overall length of 12.5 to 14.0 mm and a dioptric range of -6.00 to –16.50 D in 0.5 D increments.
Iris-Fixated Anterior Chamber PiolsThe iris-claw IOL was initially used in aphakic eyes after
intracapsular cataract extraction. Starting in 1953, the first-generation models, such as the Binkhorst and the Medallion IOLs, were associated with cystoid macular edema, corneal decompensation, lens dislocation, uveitis, and glaucoma.8 In 1978, Worst designed the iris-claw or “lobsterclaw” IOL, a coplanar single-piece PMMA IOL that was enclavated in a fold of midperipheral iris stroma, a relatively immobile portion of the iris.
Current ModelsPolymethyl methacrylate Iris-Claw Anterior Chamber p I O L : The iris-claw Artisan (Ophtec BV)/Verisyse (Abbott Medical Optics, Inc.) is a single-piece nonfoldable IOL made of Perspex CQ-UV, a UV light–filtering PMMA material. It is available for the correction of myopia, hyperopia, and astigmatism, as well as for aphakia.
The optic vaults approximately 0.87 mm anterior to the iris, providing good clearance from both the anterior lens capsule and the corneal endothelium. The distance from the optic edge to the endothelium ranges from 1.5 to 2.0 mm depending on the dioptric power, anterior chamber anatomy, and optic diameter.
Myopic pIOLs have thicker peripheral edges and therefore require more clearance than hyperopic pIOLs. The thickest part of the hyperopic IOL is central, where the ACD is greater. The toric model has a 5.0 mm optic and is available in powers ranging from +12.0 to -23.5 D in 0.5 D increments, with additional cylinder from +1.0 to +7.0 D in
Major Review
Type Material Power (D) Optic Diameter (mm) Overall Diameter (mm)Angle supported AC
Kelman Duet
Acrysof
PMMA haptic; silicone optic
Hydrophobic acrylic; 1 piece
-8 to -20
-6 to -16.5
5.5
6
12.5-13.5
12.5-14.0
Iris-Claw ACVerisyse/Artisan
Veriflex/ Artiflex
PMMA, 1 piece
PMMA Haptics,Polysiloxane optic
Myopia -3 to -15.5 Myopia -16 to -23.5Hyperopia +1 to +12Toric +12 to -23.5Torus +1 to +7
Myopia -2 to -14.5Toric -1 to -13.5Torus -1 to -5
6
6
8.5
8.5
Posterior Chamber
ICL
PRL
Collamer
Silicone
Myopia -3 to -23Torus +1 to +6Hyperopia +3 to +22
Myopia -3 to -20Hyperopia +3 to +15
4.65- 5.5
5.5
4.5 to 5.54.5
11.5 to 13
11 to 12.5
10.8 & 11.310.6
Table 1: Phakic IOLs: Important features

9www.djo.org.in
E-ISSN 0976-2892
0.5 D increments and oriented at 0 degree or at 90 degrees. The phakic Artisan/Verisyse has a fixed overall length of 8.5 mm (7.5 mm for pediatric implantations or small eyes), which is a great advantage to the surgeon who does not wish to deal with sizing measurements.
Another major advantage of these pIOLs is that they can be properly centered over the pupil, even when the pupil is off center, a relatively common situation among people with high ametropia. Off-center pupils cannot be used as a reference for centration of symmetrical IOLs such as angle-supported and sulcus-fixated IOLs.
Foldable Iris-Claw Anterior Chamber pIOL: The foldable model of the iris-claw lens is the Artiflex (OphtecBV). It is a hydrophobic polysiloxane foldable design with a 6.0 mm optic and power ranging from –2.0 to –14.5D in 0.5Dsteps. The toric model of the Artiflex is also available in Europe. The one-size-fits-all overall diameter of 8.5 mm prevents complications due to sizing errors that may occur with angle-supported or sulcus-supported pIOLs.
Posterior Chamber Phakic IOLsOne of the first posterior chamber pIOL designs, the
“collar-button” or “mushroom” configuration, is attributed to Fyodorov in 1986.9 He developed a single-piece silicone pIOLwith a 3.2mm optic and a concave anterior surface that projected anteriorly through the pupil. The pIOL was fixated behind the iris plane by 2 haptics and had a total length of 8.0 mm. Initial complications included corneal touch, decentration, pupillary block glaucoma, iridocyclitis, and cataract formation. Since the Fyodorov pIOL, evolution in design and materials has led to the emergence of several models.
Current ModelsImplantable Collamer Lens: The implantable collamer lens (ICL) is currently the most widely used posterior chamber pIOL. It incorporates material with increased biocompatibility known as Collamer (0.2% collagen and 60% hydroxylethyl methacrylate copolymer). This material attracts deposition of a monolayer of fibronectin on the IOL surface that inhibits aqueous protein binding and makes the IOL invisible to the immune system. For models V (Version) 2 and V3, the reported complications were small percentages of pupillary block and pigmentary dispersion glaucoma.10 However, late anterior subcapsular opacities of the crystalline lens occurred in 5% to 30% of cases after 1 to 3 years of follow-up (9.2% of the FDA V3 study)11,12 and are attributed to intermittent contact between the ICL and the crystalline lens.
The current model, the Visian ICL V4, is a rectangular single-piece IOL, 7.5 to 8.0 mm wide, available in 4 overall lengths: 11.5 to 13.0 mm in 0.5 mm steps for myopic correction and 11.0 to 12.5mm in 0.5 mm steps for hyperopic correction. The optic diameter ranges from 4.65 to 5.5 mm in myopic ICLs, depending on the dioptric power. It is always 5.5 mm in hyperopic ICLs. The available power ranges from
-3.0 to -23.0 D for myopic ICLs, from +3.0 to +22.0 D for hyperopic ICLs, and with an added positive cylinder of +1.0 to +6.0 D for toric ICLs correcting myopia.
The ICL can be inserted through a 3.0 mm incision using a microinjector. It has orientation markings on its haptics, allowing control during the unfolding maneuver. The thickness is less than 50 m in the optic zone, 500 to 600 um in the haptic zone, and 100 m in the haptic footplates, which are theoretically positioned in the cilliary sulcus using a spatula specially designed for the ICL.
The basic design change of the ICL V4 addresses the vaulting. This model has an additional 0.13 to 0.21mm anterior vault due to the steeper radius of curvature of the base curve, which depends on the dioptric power. The higher vault provides a greater space between the posterior surface of the ICL and the anterior surface of the crystalline lens, which allows fluid change of nutrients and prevents contact between the ICL and the crystalline lens.
Shimizu et al13 have developed the latest model of the Visian ICL- V4c. This lens includes a 360-μm KS-Aquaport located in the center of the optic, which is designed to restore a more natural aqueous flow reducing the incidence of cataract post-operatively and eliminating the need for an iridotomy after implantation. It was seen that at 6 months, 95%, and 100% eyes were within +0.5 and +1.0D of the targeted correction, respectively. Change in manifest refraction from week 1 to month 6 was 0.06+0.28 D. No significant rise in intraocular pressure (including pupillary block) or a secondary cataract occurred in any case during the observation period.
Phakic Refractive Lens: The PRL for the correction of myopia and hyperopia is made of ultrathin, highly purified, optically clear silicone and has a concave posterior base curve with a 10.0 mm radius that mimics the anterior curvature of the crystalline lens. The central thickness is less than 0.5 mm and is constant in myopic PRLs but varies in hyperopic PRLs. Edge thickness is less than 0.2 mm and is constant in hyperopic PRLs and varies in myopic ones. The diameter of the optic is 4.5 to 5.5mm, depending on the PRL power, which ranges from -3.0 to -20.0 D (maximum correction at the spectacle plane of -28.0 D). The hyperopic PRL has an overall diameter of 10.6 mm, a 4.5 mm optic, and power ranging from +3.0 to +15.0 D.
This foldable pIOL can be inserted through a 3.2mm incision and theoretically floats on a layer of aqueous humor inside the posterior chamber, exerting no pressure on the ciliary structures and having no contact with the anterior capsule of the crystalline lens. Because this type of pIOL lacks fixation, stability of centration and rotation are concerns. Thus, this pIOL is unsuitable for the correction of astigmatism. Ultrasound biomicroscopy studies document that the PRL is located on the zonules in most cases and that contact between the PRL and the crystalline lens occurs in some ca ses. Moreover, reports of PRL dislocation into the vitreous cavity have raised doubts about the safety of these IOLs.
Phakic IOLs Major Review

10 Del J Ophthalmol 2013;24(1)
ISSN 0972-0200
Pre-operative workupThe preoperative workup for pIOL should include
manifest refraction, cycloplegic refraction, Snellen uncorrected distance visual acuity (UDVA) and corrected distance visual acuity (CDVA), pupillometry, applanation tonometry, ultrasound anterior chamber depth (ACD) measurement, corneal topography, pachymetry, central endothelial cell count (ECC), and a fundus examination.
Inclusion and Exclusion CriteriaGenerally recommended inclusion criteria include:
Age >21 years, stable refraction at least 1 year, ammetropia not correctable with excimer laser surgery, unsatisfactory vision with/intolerance of contact lenses or spectacles, irido-corneal angle >300, central ECC >2300 cells/mm2(>2500 cells/mm2 if >21 years old,>2000 if >40 years old), no anomaly of iris or pupil function, mesopic pupil size <5.0–6.0 mm
Generally recommended exclusion criteria include the following: Active disease in the anterior segment, recurrent or chronic uveitis, clinically significant cataract, previous corneal or intraocular surgery (to be evaluated), IOP >21 mm Hg or glaucoma, preexisting macular degeneration or macular pathology, abnormal retinal condition, systemic diseases (eg, autoimmune disorder, connective tissue disease, atopia, diabetes mellitus)
ACD Requirements (Measured from Endothelium)AcrySof phakic: >2.7 mmArtisan-Verisyse/Artiflex-Veriflex: 2.7 mmICL: 2.8 mm for myopia, 3.0 mm for hyperopiaPRL: 2.5 mm
Intraocular Lens Power Calculation and Diameter SelectionVan der Heijde14 and Fechner et al15 proposed the
theoretical basis of the power calculation for refractive phakic iris-claw IOLs. These principles are transferable to angle-supported IOLs. To calculate IOL power, the patient’s refraction, keratometric dioptric power at the corneal apex, and adjusted ultrasound central ACD are used. Based on this formula, the manufacturers provide nomograms or software to calculate the required pIOL power.
For posterior chamber pIOLs for calculating pIOL power, most users employ the formula proposed by Olsen et al16 which uses the patient’s refraction at the 12.0 mm spectacle plane or the vertex refraction, the corneal keratometric dioptric power at its apex, and adjusted ultrasound central ACD, also known as the effective lens position.8
The pIOL’s overall diameter depends on the ACD and should provide perfect stability, with no unnecessary compression forces on the angle that could damage the angle structures or induce pupil ovalization.
Before the development of anterior segment imaging techniques such as anterior segment optical coherence tomography (AS-OCT), ultrasound biomicroscopy (UBM), and Scheimpflug imaging, it was not possible to determine the internal diameter of the anterior chamber, the angle-to-
angle distance. This evaluation was approximate and was based on a white-to-white (WTW) measurement. The WTW distance can be measured manually (using the Holladay-Godwin gauge or a measuring caliper) or by automated technology (IOL Master [Carl Zeiss Meditec], and Orbscan II topography system [Bausch & Lomb]). Automated measurement of the WTW distance provides more precise results than manual methods. The diameter of angle-supported pIOLs is oversized 0.5 mm to 1.0 mm from the WTW measurement. Currently, with the advent of AS-OCT and UBM, the angle-to-angle distance and anterior chamber angle can be measured precisely.
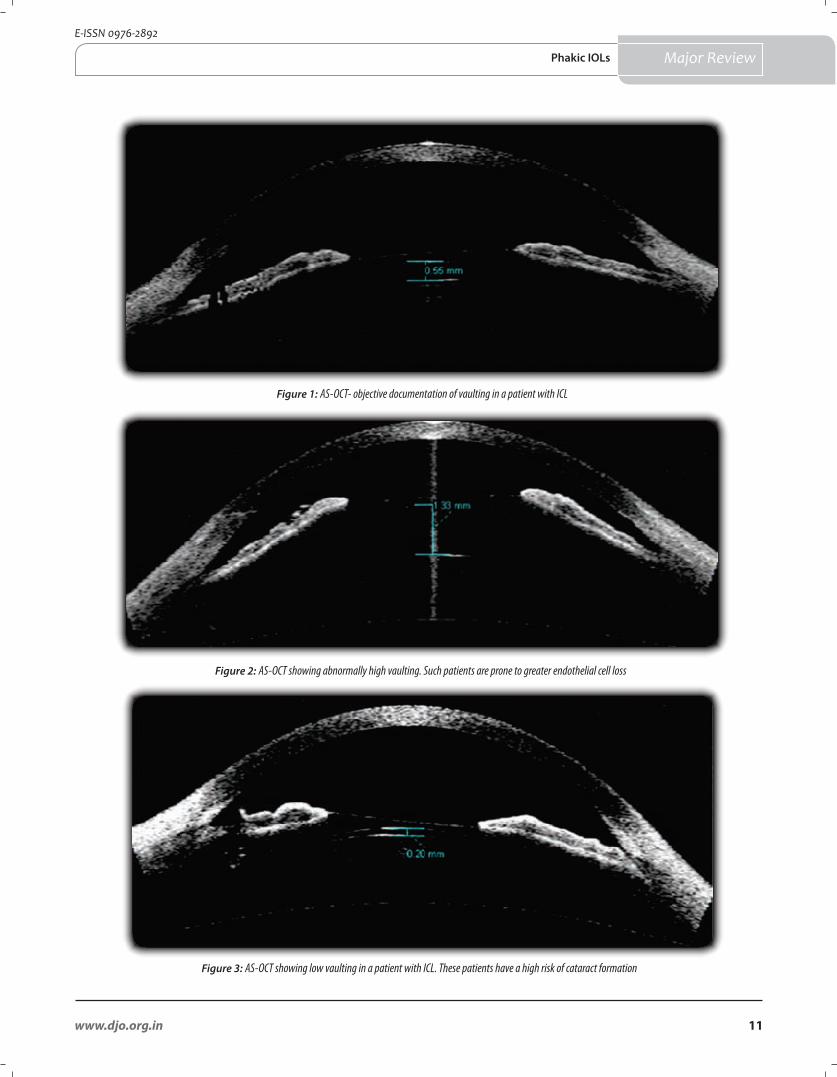
Intraocular Lens Diameter Selection: ICLThe ICL overall diameter depends on the ciliary sulcus
diameter and should provide perfect stability with no excess of compression forces to the sulcus and allow correct vaulting (Figure 1). Excessive vaulting (>750 m) due to an ICL (Figure 2) that is too long may cause angle-closure, papillary block glaucoma, or pigmentary dispersion glaucoma. Insufficient vaulting (< 250 m) due to an ICL (Figure 3) that is too short increases the risk for cataractogenesis due to the contact between the posterior surface of the ICL and the anterior surface of the crystalline lens. Before the development of UBM, no system that allowed determination of the internal diameter of the ciliary sulcus existed. This evaluation was approximated and depended on a WTW measurement. The ICL’s diameter is oversized 0.5 to 1.0 mm from the WTW measurement in myopic eyes and the same length or oversized 0.5 mm in hyperopic eyes.
However, recent studies demonstrate that there is no anatomical correspondence between external measurements and internal dimensions. Therefore, WTW distance alone may not predict angle or sulcus size, causing some of the problems experienced with anterior chamber angle-supported or posterior chamber pIOLs.
Post-operative assessment: Follow-up examinations are typically scheduled at 1 day, 1 week, 1 month, 2 months, 6 months, and 1 year after surgery and yearly thereafter. Postoperative examinations should include slit-lamp biomicroscopy, (Figure 4) keratometry, applanation tonometry, subjective and objective refraction, and measurement of uncorrected visual acuity (UCVA), BSCVA, and ECD (beginning at 6 months after surgery). Assessment of vaulting is important in cases of ICL.
Various methods have been used to assess vaulting in the post-operative period:1. Slit lamp examination: Slit lamp examination is a
subjective method and is limited in its ability to accurately determine the lens vault and cannot measure the dynamic relations during accommodation or changes in pupil size.
2. Ultrasound Biomicroscopy: Ultrasound biomicro-scopy (UBM) can be used to measure the lens vault, but certain limitations exist, such as relatively low axial
Tinwala, Titiyal.Major Review
11www.djo.org.in
E-ISSN 0976-2892
Phakic IOLs Major Review
Figure 2: AS-OCT showing abnormally high vaulting. Such patients are prone to greater endothelial cell loss
Figure 3: AS-OCT showing low vaulting in a patient with ICL. These patients have a high risk of cataract formation
Figure 1: AS-OCT- objective documentation of vaulting in a patient with ICL

12 Del J Ophthalmol 2013;24(1)
ISSN 0972-0200
resolution (20 m) and the need for direct contact with the eye for data acquisition. Moreover, UBM device uses a saline water bath with the patient supine, which could influence the depth of the lens vault.
3. Anterior segment Optical Coherence Tomography: AS-OCT is a noncontact, noninvasive technique originally designed to measure retinal thickness. The OCT device has an axial resolution of 10 m compared with an axial resolution of 20 m in the UBM systems. Using the OCT with the patient upright should make the results comparable to those with slit lamp observation.
Visual outcomes:Kazutaka Kamiya et al,17 assessed the 3-year clinical
outcomes of toric phakic intraocular lens (Visian ICL™; STAAR Surgical) implantation for moderate to high myopic astigmatism. The LogMAR uncorrected visual acuity and LogMAR best spectacle-corrected visual acuity were Snellen equivalents 20/16 and 20/12.5 respectively at 3 years postoperatively. At 3 year, 82% and 98% of the eyes were within 0.5 and 1.0 D, respectively, of the targeted correction.
For the AcrySof Cachet phakic IOL the four-year refractive results in 48 patients were as follows: UCVA: 97.9% at 20/40; 72.9% at 20/25; 47.9% at 20/20. BSCVA: 100% at 20/32; 97.9% at 20/25; 72.9% at 20/20; 43.8% at 20/16. Predictability: 68.1% within ±0.5D of target refraction; 89.4% within ±1.0 D.
A long-term (10 years) retrospective follow-up study for implantation of Artisan phakic IOL was done in moderate to high myopia.18 The mean spherical equivalent (SE) after 10 years was -0.70 + 1.00 D (range, -4.00 to 2.00 D), with no significant change in mean SE between 1, 6, and 10 years. At 10 years, 68.8% of all eyes were within 1.0 D of the intended correction. At 10 years, 31.2% (n=24) gained 1 or more Snellen lines of BCVA and 2.6% (n=2) lost more than 2 Snellen lines of BCVA; 93.3% reached a BCVA of 20/40 or better and 82.0% reached aUCVA of 20/40 or better.
A report by the American Academy of Ophthalmology on the basis of FDA trials in iris-fixated pIOLs revealed UCVA of >20/40 in 84%, >20/25 in 52%, and >20/20 in 31% of the 3-year cohort (n = 231). At 5 years postoperatively, UCVA was >20/40 in 95% in 1 study, but it was only 65% in a second study. At 10 years, refraction was still stable, with 93.3% reaching a BCVA of >20/40 and 82% achieving a UCVA of >20/40 (n = 89).19
A report by the American Academy of Ophthalmology on the basis of FDA trials in posterior-chamber pIOLs revealed UCVA was >20/40 in 81% and >20/20 in 41%. Overall, UCVA was better in those with lower levels of preoperative myopia: 97% had a UCVA of >20/40 if preoperative myopia was no more than -7 D, compared with 70% of eyes with preoperative myopia more than -10 D.19
Complications Of Phakic IOLsGeneral Complications of Intraocular Surgery
With the increasing use of topical or parabulbar anesthesia, complications due to anesthesia such as
retrobulbar hemorrhage, penetration of the globe, or life-threatening systemic side effects from accidental injection into the optic nerve are very rare. Because implantation of a pIOL is an intraocular procedure, it bears a potential risk for the development of postoperative endophthalmitis. The risk for this complication in general cataract surgery with implantation of a posterior chamber IOL is 0.1% to 0.7% with an optimal antiseptic perioperative treatment regimen.20
Changes in vaulting with accommodation, age and timeBiometric modifications of the anterior segment with
accommodation and age using anterior chamber. OCT have been performed by Baikoff et al.21 and confirm the Helmholtz theory of accommodation. With every diopter of accommodation, the anterior pole of the crystalline lens moves 30 m forward; i.e. a decrease in the distance between the posterior surface of the ICL and the anterior surface of the crystalline lens has been documented. With iris-claw pIOLs, the distance between the pIOL and the crystalline lens remains stable during accommodation, although one report observed a decrease in the space between the posterior surface of an iris-claw pIOL22 Morphologic changes of the crystalline lens with aging may also affect its relationship with pIOLs.21 Baikoff et al.’s21 observations of aging showed that along with thickening of the crystalline lens, there is forward movement of the crystalline lens’ anterior pole, even when the eye is at rest. This is accompanied by a reduction in ACD.
Kojima T et al23 evaluated the changes in vault over time after ICL implantation. Patients were divided into three groups based on vault (low < or =0.25 mm, moderate >0.25 to <0.75 mm, or high > or =0.75 mm). A significant decrease in vault was noted up to 1 month, after which the value stabilized (P<.0001). High vault showed a gradual decrease up to 3 months (P<.0001), after which the value stabilized. A statistically significant correlation was present between the change noted for vault values during the 1-year follow-up period and those measured for the initial vault on postoperative day 1 (P<.0001)
Loss of Corneal Endothelial CellsPreoperative examination should exclude patients
with low corneal endothelial cell counts or with shallow anterior chambers because the risk to corneal endothelial cells increases as the distance between the pIOL and the endothelium decreases. In a study of the new flexible anterior chamber pIOL by Baikoff et al.,14 the corneal endothelial cell loss 1year after implantation of the Vivarte pIOL was less than 5.0%, but there was a difference between the loss in myopic eyes (2.3%) and that in hyperopic eyes (5.4%). For the AcrySof foldable anterior chamber pIOL, the corneal endothelial cell loss was 4.8% after a 1-year follow-up.15
In various studies of the ICL, immediate corneal endothelial cell loss of 5.2% to 5.5% was documented after 12 months. However, the pace of corneal endothelial
Major Review Tinwala, Titiyal.

13www.djo.org.in
E-ISSN 0976-2892
Major Review
cell loss slowed down substantially from 1 year to 2 years (6.6% to 7.9%).16 Researchers therefore considered surgery to be the cause of the early corneal endothelial cell loss. Four years postoperatively, corneal endothelial cell counts showed further decrease in cell density, which may be due to the implanted ICL, the learning curve of the surgeon, or natural cell loss, which is in the range of 0.5% in the normal population.16
Pupil Ovalization / Iris Retraction Ovalization of the pupil is a specific complication
of anterior chamber pIOLs. The position of haptics in the sclerocorneal angle and their size might lead to mild deformation of the iridosclerocorneal architecture, resulting in iris retraction and pupil ovalization.
Topical use of miotic agents should be considered in the early postoperative phase if pupil ovalization associated with glare is detected. Minor pupil ovalization requires observation only, but gross ovalization indicates entrapment of the iris root and ovalization may become irreversible if the pIOL is not explanted promptly.
In contrast to anterior chamber pIOLs, no cases of pupil ovalization or iris retraction have been reported to date with posterior chamber pIOLs.
Optical Quality, Glare, Halos One disadvantage of anterior chamber pIOLs is that
they are positioned in front of the pupil, with edge effects a potential source of optical aberrations. Furthermore, the relationship between pupil size and the center of the pIOL optic is a crucial factor that should be evaluated preoperatively. Sometimes the anterior chamber pIOL optic center and the pupil center are not coincident. If the scotopic pupil size is significantly larger than the optic of the pIOL, one should be very cautious about implanting a pIOL because it will probably result in postoperative glare and subjective discomfort. In posterior chamber pIOL, due to a small optic diameter (ICL up to 5.5 mm; PRL up to 5.0 mm) and decentration of posterior chamber pIOLs in relation to the pupil size result in glare and halos, especially at night. To avoid this complication, a preoperative mesopic pupil larger than 5.0 mm should be considered a limitation.
Pigment Dispersion or Intraocular Lens DepositsAlthough no incidence of pigment dispersion or
deposits on the anterior chamber phakic IOL are reported, these conditions are seen in clinical practice. However, they do not usually negatively affect visual acuity and, thus, no further procedure is required.
Using ultrasound biomicroscopy (UBM), contact between posterior chamber pIOLs and the posterior surface of the iris has been shown. Eyes with pigment dispersion must be kept under observation to spot any increase in IOP.
Chronic Inflammation or Uveitis As anterior chamber pIOLs are positioned directly in
front of the iris, chronic inflammation and development
of pigment dispersion is possible as pupil movement can induce some friction with the pIOL.
Intraocular Pressure Elevation/Pupillary Block GlaucomaThe risk for acute pupillary block glaucoma is well
known from aphakic anterior chamber IOLs; therefore, a peripheral iridectomy is recommended. (Figure 5) Two steps are recommended to prevent acute papillary block glaucoma for angle-supported and other types of pIOLs. The entire ophthalmic viscosurgical device (OVD) must be removed from the anterior segment at the end of surgery. In addition, a preoperative iridotomy using a laser or an intraoperative surgical iridectomy to forestall acute pupillary block glaucoma is mandatory
Menezo et al24 report a statistically insignificant IOP increase of 1.5 mm Hg over 3 years after ICL implantation. Park et al8 did not find an IOP increase over 1 to 18 months after toric ICL implantation. Due to the position of the posterior chamber pIOL, the iris may be pushed forward and cause acute pupillary block glaucoma, especially in hyperopic eyes. The diameter of posterior chamber pIOLs is involved in this pathophysiological process. To prevent pupillary block glaucoma, preoperative or intraoperative iridotomies or iridectomies should be performed. In some cases, preoperative iridotomies become nonpermeable over time because they are too small or the haptic of the posterior chamber pIOL blocks them. This may cause acute pupillary block glaucoma. A second iridotomy has to be performed in these cases.
Phakic Intraocular Lens Rotation Rotation of an anterior chamber pIOL might occur
because of undersizing. Allemann et al25 report that 80% of eyes showed greater than 15 degrees of rotation by 2 years; in 60% the rotation occurred between 1 year and 2 years, implying some instability in the anterior chamber. However, IOL rotation was not associated with any clinical sequelae in these cases.1
For posterior chamber pIOLs, it is mandatory to properly measure the white-to-white (WTW) distance to choose a pIOL with sufficient length to prevent decentration or rotation, even though limitations regarding the WTW distance relative to the sulcus diameter are well known. A study reports that postoperative rotation after toric ICL implantation was less than 5 degrees in 74% of eyes and less than 11% after 8 months.8
Cataractogenesis As the position of anterior chamber pIOLs is away
from the lens, the formation of cataract is less significant than with a posterior chamber pIOL. The total incidence of cataract formation for anterior chamber pIOLs was 1.3%. The overall incidence of cataract formation for posterior chamber pIOLs was 9.60%, which is significantly higher than the incidence for anterior chamber pIOLs and iris-fixated pIOLs. Cataracts after ICL and PRL implantation often remain stable over a long period of time and rarely
Phakic IOLs

14 Del J Ophthalmol 2013;24(1)
ISSN 0972-0200
Major Review
lead to a reduction in visual acuity. The most common type of cataract after posterior chamber pIOL implantation is anterior subcapsular. Possible reasons are operative trauma, continuous or intermittent contact of the posterior chamber pIOL with the crystalline lens, insufficient nutrition through anterior chamber flow between the posterior chamber pIOL and the crystalline lens, or chronic subclinical inflammation with disruption of the blood–aqueous barrier due to friction between the pIOL and posterior iris or the haptic on the ciliary sulcus.
Retinal Detachment Ruiz-Moreno et al26 report a retinal detachment (RD)
rate of 4.8%, 1 to 44 months after anterior chamber pIOL implantation. In this study, no correlation between axial length and the incidence of RD was reported.
The largest series of RD after posterior chamber pIOL surgery was published by Martõnez-Castillo et al27 and included 16 eyes after ICL implantation (ICMV2, ICMV3, and ICMV4). In this retrospective study, RD occurred from 1 to 70 months after lens surgery (mean 29 months) and no giant retinal tear or retinal dialysis was noted. As mean axial length of the 16 eyes was 30.1 mm, the authors conclude that these RDs were part of the natural history of RD in high myopia.
ConclusionProgress is still needed on several points including the
surgeon’s learning curve and experience in sorting out intra-operative difficulties, the biocompatibility of the material, the lens design in order to achieve adequate vaulting, or at least to leave the edge of the optic at a safe distance from the endothelium and from the crystalline lens, the smooth, uniform distribution of minimal pressures at the fixating points without losing intraocular stability, the performance of the optic (fine quality of the surfaces, physiological geometry and diameter wide enough to match the patient’s scotopic pupil diameter), the lens sizing, to improve the stability of the implant
When these aims have all been achieved, current minimally invasive techniques of phakic IOL implantation are likely to produce excellent results in terms of precision, predictability and stability of the refractive outcome, with acceptable postoperative complication rates.
Financial & competing interest disclosureThe authors do not have any competing interests in any product/
procedure mentioned in this study. The authors do not have any financial interests in any product / procedure mentioned in this study
References
1. Gu¨ell JL, Rodriguez-Arenas AF, Gris O, Malecaze F, Velasco F. Phacoemulsification of the crystalline lens and implantation of an intraocular lens for the correction of moderate and high myopia: four-year follow up. J Cataract Refract Surg 2003; 29:34–8.
2. Fernandez-Vega L, Alfonso JF, Villacampa T. Clear lens extraction for the correction of high myopia. Ophthalmology 2003; 110:2349–54.
3. Strampelli B. Sopportabilita’ di lenti acriliche in camera anterior nella afachia e nei vizi di refrazione [Tolerance of acrylic lenses in the anterior chamber in aphakia and refraction disorders]. Ann Ottalmol Clin Oculist 1954; 80:75–82
4. Barraquer J. Anterior chamber plastic lenses. Results of and conclusions from five years’ experience. Trans Ophthalmol Soc UK 1959; 79:393–421; discussion 421–424
5. Ardjomand N, Ko¨ lli H, Vidic B, El-Shabrawi Y, Faulborn J. Pupillary block after phakic anterior chamber intraocular lens implantation. J Cataract Refract Surg 2002; 28:1080–1.
6. Apple DJ, Brems RN, Park RB, Kavka-Van Norman D,Hansen SO, Tetz MR, Richards SC, Letchinger SD. Anterior chamber lenses. Part I: complications and pathology and a review of designs. J Cataract Refract Surg 1987; 13:157–74.
7. Alio´ JL, Pin˜ero D, Bernabeu G, Galal A, Vargas JM, Ismail MM. The Kelman Duet phakic intraocular lens: 1-year results. J Refract Surg 2007; 23:868–79.
8. Lovisolo CF, Reinstein DZ. Phakic intraocular lenses. Surv Ophthalmol 2005; 50:549–87.
Figure 5: Pre-operative ND-YAG laser peripheral iridotomy
Figure 4: Slit lamp examination demonstrating ICL vaulting
Tinwala, Titiyal.

15www.djo.org.in
E-ISSN 0976-2892
Major Review
9. Fyodorov SN, Zuyev VK, Aznabayev BM. [Intraocular correction of high myopia with negative posterior chamber lens]. [Russian] Oftalmokhirurgiia 1991; 3:57–8.
10. Kodjikian L,Gain P,Donate D, Rouberol F,Burillon C.Malignant glaucoma induced by a phakic posterior chamber intraocular lens for myopia. J Cataract Refract Surg 2002; 28:2217–21.
11. Menezo JL, Peris-Martı´nez C, Cisneros-Lanuza AL, Martı´nez-Costa R. Rate of cataract formation in 343 highly myopic eyes after implantation of three types of phakic intraocular lenses. J Refract Surg 2004; 20:317–24.
12. Sanders DR, Vukich JA. Incidence of lens opacities and clinically significant cataracts with the Implantable Contact Lens: comparison of two lens designs; the ICL in Treatment of Myopia (ITM) Study Group. J Refract Surg 2002; 18:673–82.
13. Kimiya Shimizu, Kazutaka Kamiya, Akihito Igarashi, Tetsu Shiratani. Early clinical outcomes of implantation of posterior chamber phakic intraocular lens with a central hole (Hole ICL) for moderate to high myopia. Br J Ophthalmol 2012; 96:409-12.
14. Van der Heijde GL. Some optical aspects of implantation of an IOL in amyopic eye.Eur J Implant Refract Surg 1989; 1:245–248 63.
15. Fechner PU, van der Heijde GL, Worst JGF. The correction of myopia by lens implantation into phakic eyes. Am J Ophthalmol 1989; 107:659–63.
16. Olsen T, Corydon L, Gimbel H. Intraocular lens power calculation with an improved anterior chamber depth prediction algorithm. J Cataract Refract Surg 1995; 21:313–19.
17. Kamiya K, Shimizu K, Kobashi H, Igarashi A, Komatsu M (2013) Three-Year Follow-Up of Posterior Chamber Toric Phakic Intraocular Lens Implantation for Moderate to High Myopic Astigmatism. PLoS ONE 8(2): e56453.
18. Tahzib NG, Nuijts RMMA, Wu WY, Budo CJ. Ophthalmology. 2007; 114(6):1133-42.
19. David Huang, MD, PhD, Steven C. Schallhorn, MD, Alan Sugar, MD, MS, Ayad A. Farjo, MD,Parag A. Majmudar, MD, William B. Trattler, MD, David J. Tanzer, MD. Phakic Intraocular Lens Implantation for the Correction of Myopia:A Report by the American Academy of Ophthalmology; Ophthalmology 2009; 116:2244–58.
20. Fechner PU, Worst JGF.A new concave intraocular lens for the correction of myopia. Eur J Implant Refract Surg 1989; 1:41–3.
21. Baikoff G, Lutun E, Ferraz C, Wei J. Static and dynamic analysis of the anterior segment with optical coherence tomography. J Cataract Refract Surg 2004; 30:1843–50.
22. Baikoff G, Lutun E, Wei J, Ferraz C. Contact between 3 phakic intraocular lens models and the crystalline lens: an anterior chamber optical coherence tomography study. J Cataract Refract Surg 2004; 30:2007–12.
23. Kojima T, Maeda M, Yoshida Y, Ito M, Nakamura T, Hara S, Ichikawa K. Posterior chamber phakic implantable collamer lens: changes in vault during 1 year. J Refract Surg 2010; 26(5):327-32.
24. Fink AM, Gore C, Rosen ES. Refractive lensectomy for hyperopia.Ophthalmology 2000; 107:1540–8.
25. Stulting RD, John ME, Maloney RK, Assil KK, Arrowsmith PN, Thompson VM. Three-year results of Artisan/Verisyse phakic intraocular lens implantation; results of the United States Food and Drug Administration Clinical Trial; the U.S. Verisyse Study Group. Ophthalmology 2008; 115:464–72.
26. Landesz M, Worst JGF, van Rij G. Long-term results of correction of high myopia with an iris claw phakic intraocular lens. J Refract Surg 2000; 16:310–6.
27. Baikoff G, Lutun E, Wei J, Ferraz C. Anterior chamber optical coherence tomography study of human natural accommodation in a 19-year-old albino. J Cataract Refract Surg 2004; 30:696–701.
Phakic IOLs
Early Bird Registration Deadline 31 August, 2013For latest updates log on to
www.arvo.org/Conferences_and_Courses/Asia-ARVO/2013/Welcome/www.asiaarvo2013.org/accommodation.htm
16 Del J Ophthalmol 2013;24(1)
ISSN 0972-0200
Intra-Stromal Corneal Ring SegmentsDelhi J Ophthalmol 2013; 24 (1): 16-22
Intra-stromal corneal ring segments (ICRS) are a new modality in the treatment of corneal ectactic disorders like keratoconus, post lasik ectasia and pellucid marginal degeneration. ICRS is a minimally invasive technique wherein the central optical zone is not disturbed with long term convenient refractive correction. Two brands of ICRS segments are popular commercially, Intacs (Additions Technology Inc) and Ferrara Rings. ICRS reduces the sphere, cylinder and the spherical equivalent in keratoconus. Pre-operative evaluation and patient selection plays a key role in the success of the implant. The determination of which segment to implant depends upon pre-operative manifest refraction, spherical equivalent, location of the cone and degree of asymmetric astigmatism. ICRS along with collagen cross linking has opened new vistas in the treatment of keratoconus and corneal ectasia. While cross linking stops the progression of the ectasia and reverses it to some extent, ICRS flatten or normalize the corneal shape. Combining both the modalities together has a synergistic action and can be performed simulatneously or sequentially. Complications are rare as ICRS implantation is reversible, no corneal tissue is removed, and the central optical zone is not invaded.
*Ramendra Bakshi, Charu Khurana, Ritika SachdevMahipal SachdevConsultant Cornea & Refractive Surgery, Centre for Sight, B5/24, Safdarjung Enclave, New Delhi
*Address for correspondence
Introduction Corneal ectatic diseases such
as Keratoconus, Pellucid Marginal Degeneration and Post Lasik Ectasia may impair vision severely leading to decline in both uncorrected and best corrected visual acuity. In a large proportion of patients the cornea is affected to an extent that once the patient is not able to use rigid contact lenses, there are few surgical alternatives for correction. Expectations are limited, and the anatomic and functional results can be unpredictable. Previously, Penetrating Keratoplasty was the treatment of choice.
Although corneal transplant (penetrating or lamellar) can be very successful in this subset of patients, limitations of it can include high post-op cylinder, side effects from chronic topical steroids, corneal rejection, and recurrence of keratoconus in the donor cornea. Intra-stromal corneal ring segments (ICRS) are a new modality in the treatment of mild to moderate grades of such corneal ectactic disorders.
HistoryICRS implantation is a minimally
invasive, tissue saving surgical procedure
that can be used to treat keratoconic corneas. Several studies have also shown the efficacy of ICRS in treating many other corneal conditions, such as post-lasik ectasia, astigmatism and myopia.1-4 The ICRS concept was proposed by Reynolds in 1978.5 It was first evaluated for the treatment of Myopia by Keravision.6 Intacs technology for myopia received FDA approval in 1999. This technology was then adopted for the treatment of keratoconus.7 Colin et al were the first to report the use of these rings in keratoconus. They found Intacs reduced the corneal steepening and astigmatism associated with keratoconus.8
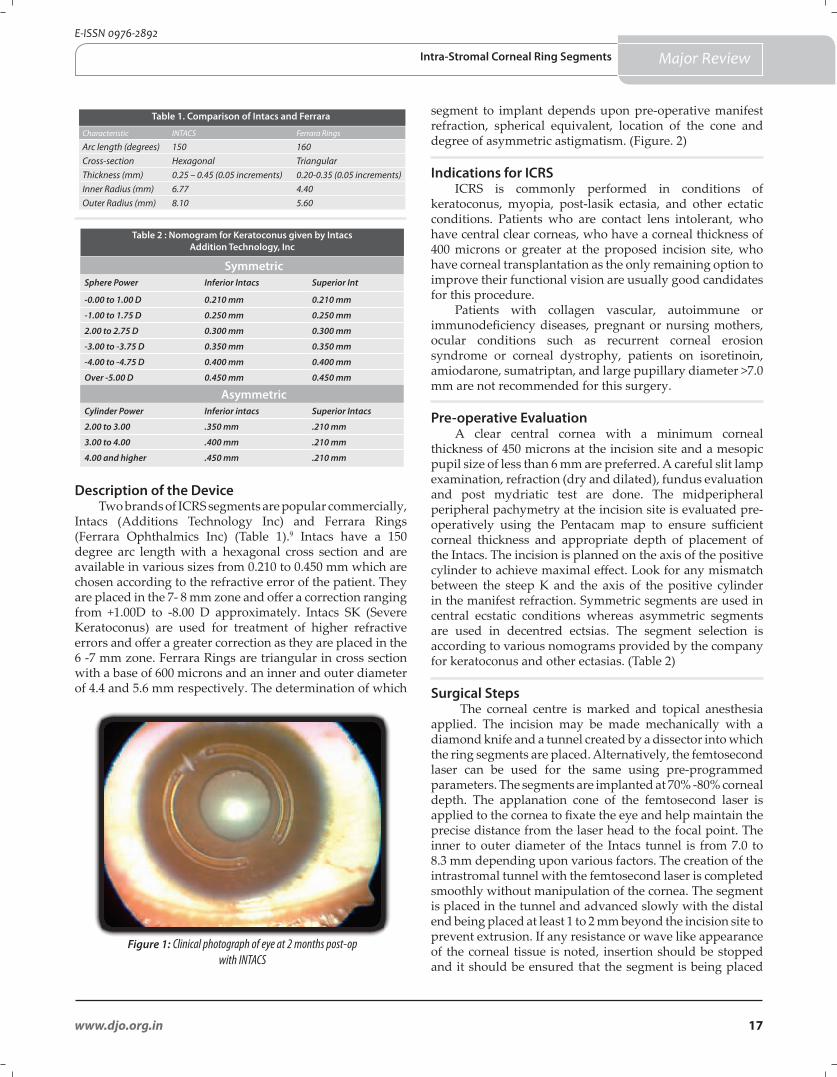
Principle ICRS consist of two, tiny clear
crescent shapes pieces of PMMA which can be inserted into the cornea (Figure.1). For myopia, ICRS work by flattening the cornea to re-focus light rays and improve vision while in keratoconus patients, ICRS flatten the steep part of the cone and reduce vision distortions. Based on the principle of the ‘hammock effect’, they redistribute the bio-mechanical stress and prevent further steepening of the cornea.
Keywords : Intra-stromal corneal ring segments • keratoconus • post lasik ectasia • Intacs
Ramendra Bakshi MS, FRCS
Centre for Sight, B5/24, Safdarjung Enclave, New Delhi. email: [email protected]
Major Review
DOI: http://dx.doi.org/10.7869/djo.2013.3
17www.djo.org.in
E-ISSN 0976-2892
Characteristic INTACS Ferrara Rings
Arc length (degrees) 150 160Cross-section Hexagonal TriangularThickness (mm) 0.25 – 0.45 (0.05 increments) 0.20-0.35 (0.05 increments)Inner Radius (mm) 6.77 4.40Outer Radius (mm) 8.10 5.60
Table 1. Comparison of Intacs and Ferrara
Table 2 : Nomogram for Keratoconus given by Intacs Addition Technology, Inc
SymmetricSphere Power Inferior Intacs Superior Int
-0.00 to 1.00 D 0.210 mm 0.210 mm
-1.00 to 1.75 D 0.250 mm 0.250 mm
2.00 to 2.75 D 0.300 mm 0.300 mm
-3.00 to -3.75 D 0.350 mm 0.350 mm
-4.00 to -4.75 D 0.400 mm 0.400 mm
Over -5.00 D 0.450 mm 0.450 mm
AsymmetricCylinder Power Inferior intacs Superior Intacs
2.00 to 3.00 .350 mm .210 mm
3.00 to 4.00 .400 mm .210 mm
4.00 and higher .450 mm .210 mm
Figure 1: Clinical photograph of eye at 2 months post-op with INTACS
Description of the Device Two brands of ICRS segments are popular commercially,
Intacs (Additions Technology Inc) and Ferrara Rings (Ferrara Ophthalmics Inc) (Table 1).9 Intacs have a 150 degree arc length with a hexagonal cross section and are available in various sizes from 0.210 to 0.450 mm which are chosen according to the refractive error of the patient. They are placed in the 7- 8 mm zone and offer a correction ranging from +1.00D to -8.00 D approximately. Intacs SK (Severe Keratoconus) are used for treatment of higher refractive errors and offer a greater correction as they are placed in the 6 -7 mm zone. Ferrara Rings are triangular in cross section with a base of 600 microns and an inner and outer diameter of 4.4 and 5.6 mm respectively. The determination of which
segment to implant depends upon pre-operative manifest refraction, spherical equivalent, location of the cone and degree of asymmetric astigmatism. (Figure. 2)
Indications for ICRSICRS is commonly performed in conditions of
keratoconus, myopia, post-lasik ectasia, and other ectatic conditions. Patients who are contact lens intolerant, who have central clear corneas, who have a corneal thickness of 400 microns or greater at the proposed incision site, who have corneal transplantation as the only remaining option to improve their functional vision are usually good candidates for this procedure.
Patients with collagen vascular, autoimmune or immunodeficiency diseases, pregnant or nursing mothers, ocular conditions such as recurrent corneal erosion syndrome or corneal dystrophy, patients on isoretinoin, amiodarone, sumatriptan, and large pupillary diameter >7.0 mm are not recommended for this surgery.
Pre-operative Evaluation A clear central cornea with a minimum corneal
thickness of 450 microns at the incision site and a mesopic pupil size of less than 6 mm are preferred. A careful slit lamp examination, refraction (dry and dilated), fundus evaluation and post mydriatic test are done. The midperipheral peripheral pachymetry at the incision site is evaluated pre-operatively using the Pentacam map to ensure sufficient corneal thickness and appropriate depth of placement of the Intacs. The incision is planned on the axis of the positive cylinder to achieve maximal effect. Look for any mismatch between the steep K and the axis of the positive cylinder in the manifest refraction. Symmetric segments are used in central ecstatic conditions whereas asymmetric segments are used in decentred ectsias. The segment selection is according to various nomograms provided by the company for keratoconus and other ectasias. (Table 2)
Surgical Steps The corneal centre is marked and topical anesthesia
applied. The incision may be made mechanically with a diamond knife and a tunnel created by a dissector into which the ring segments are placed. Alternatively, the femtosecond laser can be used for the same using pre-programmed parameters. The segments are implanted at 70% -80% corneal depth. The applanation cone of the femtosecond laser is applied to the cornea to fixate the eye and help maintain the precise distance from the laser head to the focal point. The inner to outer diameter of the Intacs tunnel is from 7.0 to 8.3 mm depending upon various factors. The creation of the intrastromal tunnel with the femtosecond laser is completed smoothly without manipulation of the cornea. The segment is placed in the tunnel and advanced slowly with the distal end being placed at least 1 to 2 mm beyond the incision site to prevent extrusion. If any resistance or wave like appearance of the corneal tissue is noted, insertion should be stopped and it should be ensured that the segment is being placed
Major ReviewIntra-Stromal Corneal Ring Segments
18 Del J Ophthalmol 2013;24(1)
ISSN 0972-0200
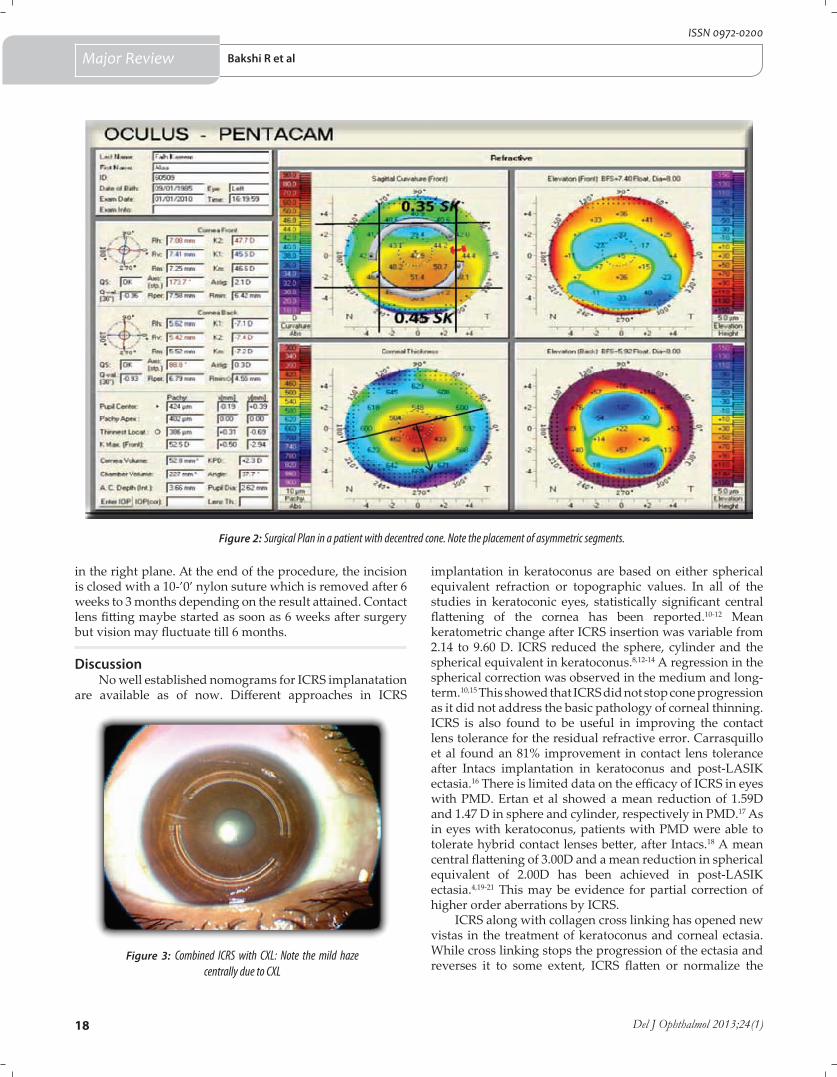
Figure 2: Surgical Plan in a patient with decentred cone. Note the placement of asymmetric segments.
Figure 3: Combined ICRS with CXL: Note the mild haze centrally due to CXL
in the right plane. At the end of the procedure, the incision is closed with a 10-’0’ nylon suture which is removed after 6 weeks to 3 months depending on the result attained. Contact lens fitting maybe started as soon as 6 weeks after surgery but vision may fluctuate till 6 months.
DiscussionNo well established nomograms for ICRS implanatation
are available as of now. Different approaches in ICRS
implantation in keratoconus are based on either spherical equivalent refraction or topographic values. In all of the studies in keratoconic eyes, statistically significant central flattening of the cornea has been reported.10-12 Mean keratometric change after ICRS insertion was variable from 2.14 to 9.60 D. ICRS reduced the sphere, cylinder and the spherical equivalent in keratoconus.8,12-14 A regression in the spherical correction was observed in the medium and long-term.10,15 This showed that ICRS did not stop cone progression as it did not address the basic pathology of corneal thinning. ICRS is also found to be useful in improving the contact lens tolerance for the residual refractive error. Carrasquillo et al found an 81% improvement in contact lens tolerance after Intacs implantation in keratoconus and post-LASIK ectasia.16 There is limited data on the efficacy of ICRS in eyes with PMD. Ertan et al showed a mean reduction of 1.59D and 1.47 D in sphere and cylinder, respectively in PMD.17 As in eyes with keratoconus, patients with PMD were able to tolerate hybrid contact lenses better, after Intacs.18 A mean central flattening of 3.00D and a mean reduction in spherical equivalent of 2.00D has been achieved in post-LASIK ectasia.4,19-21 This may be evidence for partial correction of higher order aberrations by ICRS.
ICRS along with collagen cross linking has opened new vistas in the treatment of keratoconus and corneal ectasia. While cross linking stops the progression of the ectasia and reverses it to some extent, ICRS flatten or normalize the
Major Review Bakshi R et al
19www.djo.org.in
E-ISSN 0976-2892
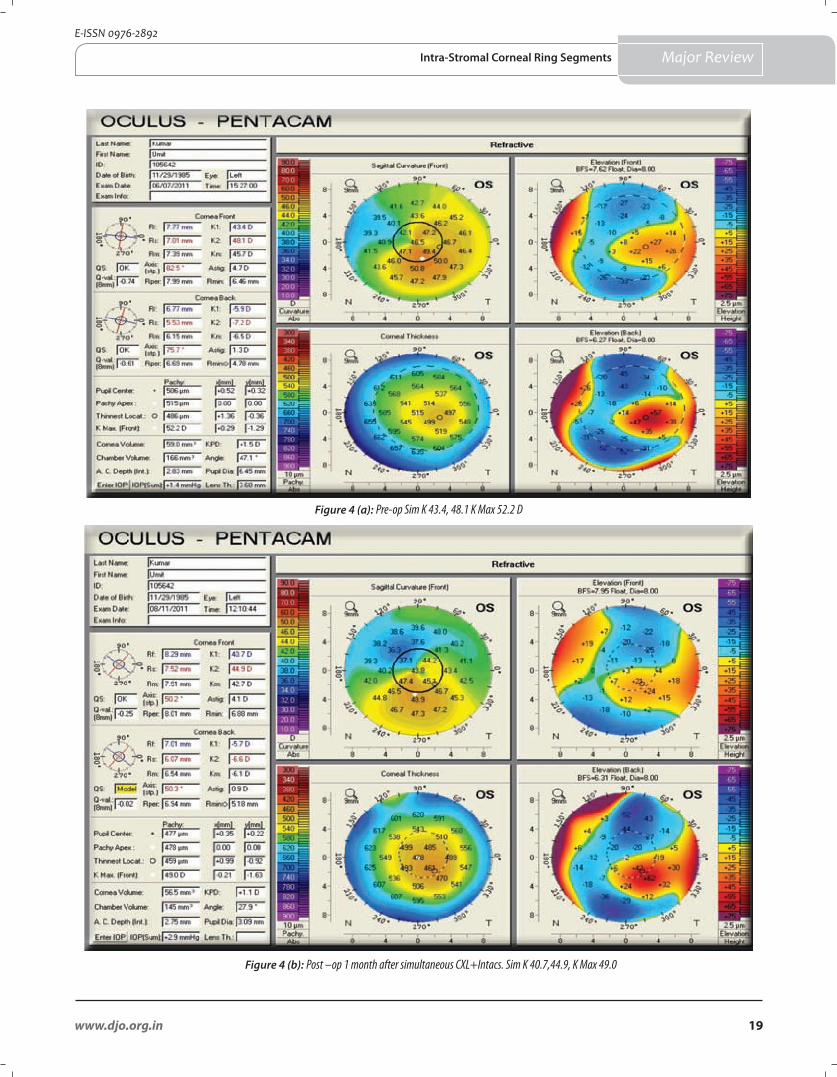
Figure 4 (a): Pre-op Sim K 43.4, 48.1 K Max 52.2 D
Figure 4 (b): Post –op 1 month after simultaneous CXL+Intacs. Sim K 40.7,44.9, K Max 49.0
Major ReviewIntra-Stromal Corneal Ring Segments
20 Del J Ophthalmol 2013;24(1)
ISSN 0972-0200
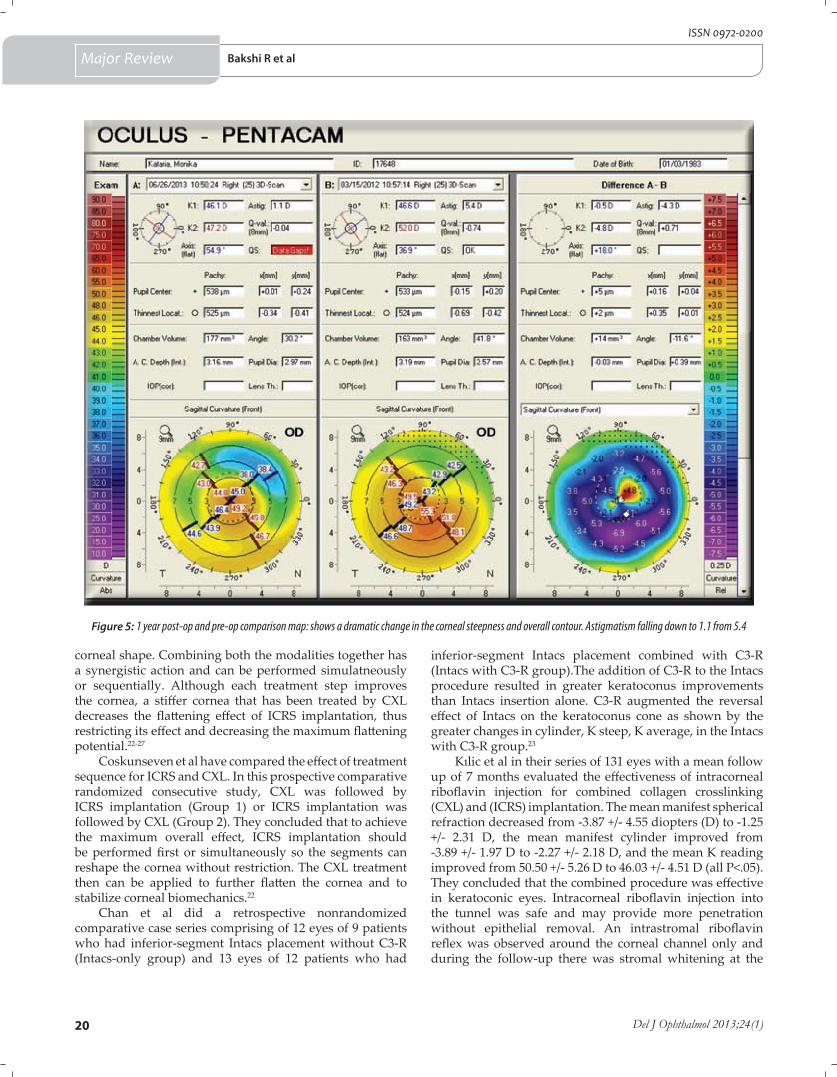
Figure 5: 1 year post-op and pre-op comparison map: shows a dramatic change in the corneal steepness and overall contour. Astigmatism falling down to 1.1 from 5.4
corneal shape. Combining both the modalities together has a synergistic action and can be performed simulatneously or sequentially. Although each treatment step improves the cornea, a stiffer cornea that has been treated by CXL decreases the flattening effect of ICRS implantation, thus restricting its effect and decreasing the maximum flattening potential.22-27
Coskunseven et al have compared the effect of treatment sequence for ICRS and CXL. In this prospective comparative randomized consecutive study, CXL was followed by ICRS implantation (Group 1) or ICRS implantation was followed by CXL (Group 2). They concluded that to achieve the maximum overall effect, ICRS implantation should be performed first or simultaneously so the segments can reshape the cornea without restriction. The CXL treatment then can be applied to further flatten the cornea and to stabilize corneal biomechanics.22
Chan et al did a retrospective nonrandomized comparative case series comprising of 12 eyes of 9 patients who had inferior-segment Intacs placement without C3-R (Intacs-only group) and 13 eyes of 12 patients who had
inferior-segment Intacs placement combined with C3-R (Intacs with C3-R group).The addition of C3-R to the Intacs procedure resulted in greater keratoconus improvements than Intacs insertion alone. C3-R augmented the reversal effect of Intacs on the keratoconus cone as shown by the greater changes in cylinder, K steep, K average, in the Intacs with C3-R group.23
Kılic et al in their series of 131 eyes with a mean follow up of 7 months evaluated the effectiveness of intracorneal riboflavin injection for combined collagen crosslinking (CXL) and (ICRS) implantation. The mean manifest spherical refraction decreased from -3.87 +/- 4.55 diopters (D) to -1.25 +/- 2.31 D, the mean manifest cylinder improved from -3.89 +/- 1.97 D to -2.27 +/- 2.18 D, and the mean K reading improved from 50.50 +/- 5.26 D to 46.03 +/- 4.51 D (all P<.05). They concluded that the combined procedure was effective in keratoconic eyes. Intracorneal riboflavin injection into the tunnel was safe and may provide more penetration without epithelial removal. An intrastromal riboflavin reflex was observed around the corneal channel only and during the follow-up there was stromal whitening at the
Major Review Bakshi R et al

21www.djo.org.in
E-ISSN 0976-2892
References
1. Levinger S, Pokroy R. Keratoconus managed with intacs: one-year results. Arch Ophthalmol 2005; 123(10):1308-14.
2. Anil Kubaloglu et al. Comparison of mechanical and femtosecond laser tunnel creation for intrastromal corneal ring segment implantation in keratoconus. Prospective randomized clinical trial. J Cataract Refract Surg 2010; 36:1556–61.
3. Aylin Ertan et al. Intacs implantation using a femtosecond laser for management of keratoconus: Comparison of 306 cases in different stages J Cataract Refract Surg 2008.
4. Piñero DP, Alio JL, Uceda-Montanes A, El Kady B, Pascual I. Intracorneal ring segment implantation in corneas with post-laser in situ keratomileusis keratectasia.Ophthalmology 2009; 116(9):1665-74.
5. Burris TE. Intrastromal corneal ring technology: results and indications. Curr Opin Ophthalmol 1998; 9(4):9-14.
6. Twa MD, Karpecki PM, King BJ, Linn SH, Durrie DS, Schanzlin DJ. : One-year results from the phase III investigation of the KeraVision Intacs. J Am Optom Assoc 1999; 70(8):515-24.
7. Asbell PA. :Intacs corneal implants for myopia: an effective refractive alternative with proven efficacy and safety. In Clin J, Ertan A, eds. Intracorneal Ring Segments and Alternative Treatments for Corneal Ectatic diseases. Ankara: Kudret Goz, 2007; 37-48
8. Colin J, Cochener B, Savary G, Malet F. : Correcting keratoconus with intracorneal rings. J Cataract Refract Surg 2000; 26(8):1117-22.
9. Ertan A, Colin J . Intracorneal rings for keratoconus and keratectasia. J Cataract Refract Surg 2007 ; 33(7):1303-14.
10. Siganos D, Ferrara P, Chatzinikolas K, Bessis N, Papastergiou G.: Ferrara intrastromal corneal rings for the correction of keratoconus. J Cataract Refract Surg 2002; 28(11):1947-51.
11. Coskunseven E, Kymionis GD, Tsiklis NS, Atun S, Arslan E, Jankov MR, Pallikaris IG: One-year results of intrastromal corneal ring segment implantation (KeraRing) using femtosecond laser in patients with keratoconus. Am J Ophthalmol 2008; 145(5):775-9.
12. Ertan A, Kamburoğlu G :Intacs implantation using a femtosecond laser for management of keratoconus: Comparison of 306 cases in different stages. J Cataract Refract Surg 2008; 34(9):1521-6.
13. Kwitko S, Severo NS: Ferrara intracorneal ring segments for keratoconus. J Cataract Refract Surg 2004; 30(4):812-20.
14. 14. Alió JL, Artola A, Hassanein A, Haroun H, Galal A. : One or 2 Intacs segments for the correction of keratoconus. J Cataract Refract Surg 2005; 31(5):943-53.
15. Kymionis GD, Siganos CS, Tsiklis NS, Anastasakis A, Yoo SH, Pallikaris AI, Astyrakakis N, Pallikaris IG : Long-term follow-up of Intacs in keratoconus. Am J Ophthalmol 2007; 143(2):236-244.
16. Carrasquillo KG, Rand J, Talamo JH : Intacs for keratoconus and post-LASIK ectasia: mechanical versus femtosecond laser-assisted channel creation. Cornea 2007; 26(8):956-62.
location surrounding the segment. Limited and localized riboflavin penetration around the ICRS may increase the effect of the segments and produce less corneal haze in the central cornea, which may affect visual acuity.24 It has also be hypothesised that the newly dissected femtosecond corneal channel may result in more pooling of riboflavin with resultant exaggerated flattening effect of CXL. This is in contrast to the healed channel that was potentially closed tightly on the ring.25-27 In our experience of 36 eyes of 22 patients presenting with keratoconus and post lasik ectasia underwent Simultaneous CXL with Intacs at our centre. Details of UCVA, Refraction and BCVA, Topography (Pentacam) were documented preoperatively and at post-op 3, 6 and 12 months. Intacs channels were created with the help of Femtosecond Laser and CXL was performed with the conventional epithelium-off method. Mean age was 25+/-5.08 years. Mean follow up was 8.78+/-2.1 months (range 6 -12 months). Average Sim K pre-op was 45.55+/- 3.13 D which reduced to 42.0+/-2.09 D. Average K Max pre-op 51.9+/-1.48 D which reduced to 47.0+/-1.33D post-op. Mean cylinder pre-op was 5.93 ± 3.65 which reduced to 3.13 ± 2.13. The mean sphere reduced from 6.23 ± 2.57 to 3.2 ± 2.29. (Figure 3,4 and 5) Complications noted were channel deposits in 2 eyes which responded to topical steroids and anterior chamber perforation in 1 eye for which the segment was extracted.
Complications
Complications are rare as ICRS implantation is reversible, no corneal tissue is removed, and the central optical zone is not invaded.
Intraoperative complications are epithelial defects at the keratotomy site, inadequate channel depth or dissection, superficial channel dissection, segment decentration, asymmetry of implants, and anterior chamber perforation.1-3,28,29 Postoperatively, segment extrusion, corneal neovascularization, segment migration, segment extrusion, epithelial plug at the initial incison site, infectious keratitis, channel deposits, corneal haze, corneal melting, persistent incisional gaping, night halos, chronic pain, and focal edema have been reported. 12-15,19,28,29 ICRS can easily be explanted and visual, refractive, and topographic features can return to pre-implantation values.30 Adjustment surgery can also be performed to improve visual acuity and corneal regularity.31
ConclusionsICRS is a minimally invasive technique wherein
the central optical zone is not disturbed with long term convenient refractive correction. Results are rapid & predictable with minimal visual adverse effects. The segments are removable & exchangeable. Corneal asphericity is maintained.Patients should be presented with realistic expectations to avoid disappointment. Well-designed, prospective, comparative studies are needed to establish accurate nomograms for ICRS implantation.ICRS in conjunction with CXL serves a dual purpose of halting
disease progression and normalizing the corneal shape. Improvement in UCVA & BCVA occurs in the same sitting. This has a synergistic action and is convenient for the patient as in a single sitting the procedure is complete.
Financial & competing interest disclosureThe authors do not have any competing interests in any product/
procedure mentioned in this study. The authors do not have any financial interests in any product / procedure mentioned in this study
Major ReviewIntra-Stromal Corneal Ring Segments
22 Del J Ophthalmol 2013;24(1)
ISSN 0972-0200
17. Ertan A, Bahadir M. : Intrastromal ring segment insertion using a femtosecond laser to correct pellucid marginal corneal degeneration. J Cataract Refract Surg 2006; 32(10):1710-6.
18. Rodriguez-Prats J, Galal A, Garcia-Lledo M, De La Hoz F, Alió JL.: Intracorneal rings for the correction of pellucid marginal degeneration. J Cataract Refract Surg 2003; 29(7):1421-4.
19. 19. Kymionis GD, Tsiklis NS, Pallikaris AI, Kounis G, Diakonis VF, Astyrakakis N, Siganos CS : Long-term follow-up of Intacs for post-LASIK corneal ectasia. Ophthalmology 2006; 113(11):1909-17.
20. Sharma M, Boxer Wachler BS : Comparison of single-segment and double-segment Intacs for keratoconus and post-LASIK ectasia .
21. Pokroy R, Levinger S, Hirsh A. Single Intacs segment for post-laser in situ keratomileusis keratectasia. J Cataract Refract Surg 2004; 30(8):1685-95.
22. Coskunseven et al. Effect of treatment sequence in combined intrastromal corneal rings and corneal collagen crosslinking for keratoconus. J Cataract Refract Surg 2009; 35:2084–91.
23. Chan CC Effect of inferior-segment Intacs with and without C3-R on keratoconus. J Cataract Refract Surg 2007 ; 33(1):75-80.
24. Kilic et al. Riboflavin injection into the corneal channel for combined collagen crosslinking and intrastromal corneal ring segment implantation. J Cataract Refract Surg 2012; 38(5):878-83.
25. El-Raggal TM. Effect of corneal collagen crosslinking on femtosecond laser channel creation for intrastromal corneal ring segment implantation in keratoconus. J Cataract Refract Surg 2011; 37(4):701-5.
26. Renesto Ada C et al,Sequential topical riboflavin with or without ultraviolet a radiation with delayed intracorneal ring segment insertion for keratoconus. Am J Ophthalmol 2012; 153(5):982-93.
27. Saelens IE, Refractive, topographic, and visual outcomes of same-day corneal cross-linking with Ferrara intracorneal ring segments in patients with progressive keratoconus. Cornea 2011; 30(12):1406-8.
28. Boxer Wachler BS, Christie JP, Chandra NS, Chou B, Korn T, Nepomuceno R: Intacs for keratoconus. Ophthalmology 2003; 110(5):1031-40.
29. Miranda D, Sartori M, Francesconi C, Allemann N, Ferrara P, Campos M. : Ferrara intrastromal corneal ring segments for severe keratoconus.
30. Alió JL, Artola A, Ruiz-Moreno JM, Hassanein A, Galal A, Awadalla MA. : Changes in keratoconic corneas after intracorneal ring segment explantation and reimplantation.
31. Pokroy R, Levinger S : Intacs adjustment surgery for keratoconus. J Cataract Refract Surg 2006; 32(6):986-92.
Major Review Bakshi R et al
The “Techniques” section of Delhi Journal of Ophthalmology now features a VIDEO on the DJO web page.
Please log on to www.djo.org.in to view the surgical video of the “Techniques” Section of DJO.
Dr M.VANATHI MDEditor-in-chief
Delhi Journal of Ophthalmology
Announcement
23www.djo.org.in
E-ISSN 0976-2892
Efficacy of Corneal Collagen Crosslinking with Riboflavin and Ultraviolet A in Progressive KeratoconusDelhi J Ophthalmol 2013; 24 (1): 23-27
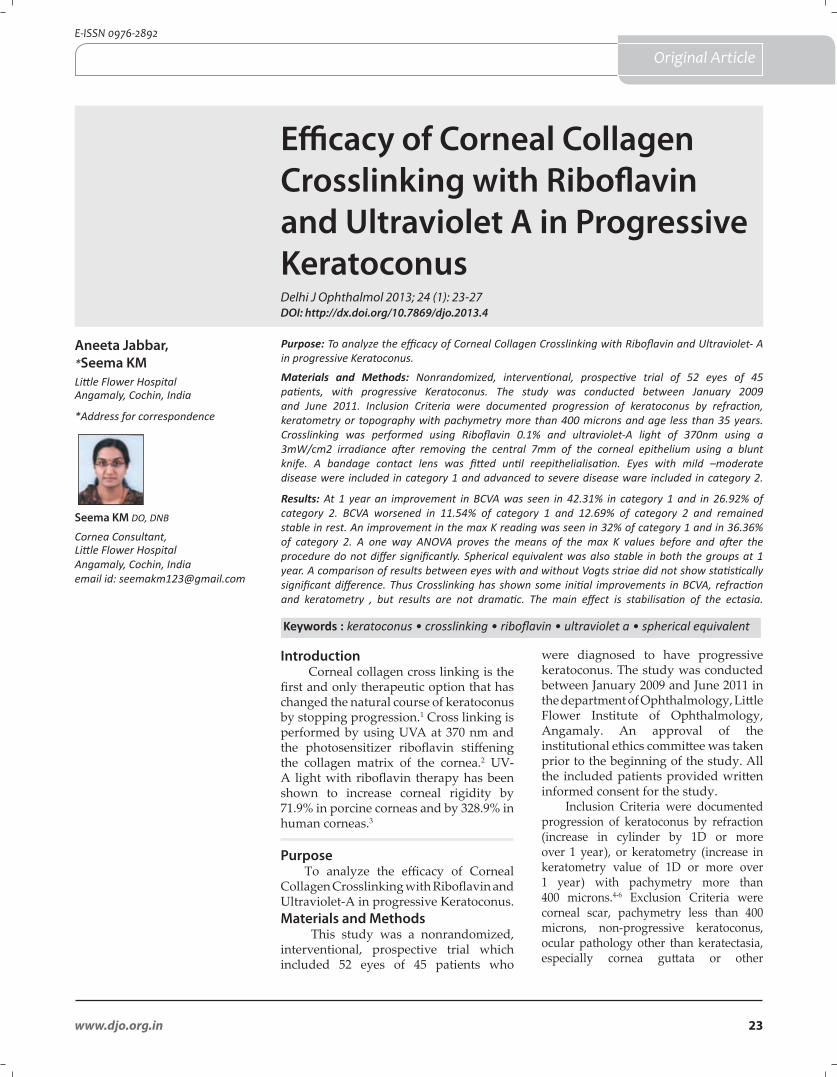
Purpose: To analyze the efficacy of Corneal Collagen Crosslinking with Riboflavin and Ultraviolet- A in progressive Keratoconus.
Materials and Methods: Nonrandomized, interventional, prospective trial of 52 eyes of 45 patients, with progressive Keratoconus. The study was conducted between January 2009 and June 2011. Inclusion Criteria were documented progression of keratoconus by refraction, keratometry or topography with pachymetry more than 400 microns and age less than 35 years. Crosslinking was performed using Riboflavin 0.1% and ultraviolet-A light of 370nm using a 3mW/cm2 irradiance after removing the central 7mm of the corneal epithelium using a blunt knife. A bandage contact lens was fitted until reepithelialisation. Eyes with mild –moderate disease were included in category 1 and advanced to severe disease ware included in category 2.
Results: At 1 year an improvement in BCVA was seen in 42.31% in category 1 and in 26.92% of category 2. BCVA worsened in 11.54% of category 1 and 12.69% of category 2 and remained stable in rest. An improvement in the max K reading was seen in 32% of category 1 and in 36.36% of category 2. A one way ANOVA proves the means of the max K values before and after the procedure do not differ significantly. Spherical equivalent was also stable in both the groups at 1 year. A comparison of results between eyes with and without Vogts striae did not show statistically significant difference. Thus Crosslinking has shown some initial improvements in BCVA, refraction and keratometry , but results are not dramatic. The main effect is stabilisation of the ectasia.
Aneeta Jabbar, *Seema KMLittle Flower HospitalAngamaly, Cochin, India
Introduction Corneal collagen cross linking is the
first and only therapeutic option that has changed the natural course of keratoconus by stopping progression.1 Cross linking is performed by using UVA at 370 nm and the photosensitizer riboflavin stiffening the collagen matrix of the cornea.2 UV- A light with riboflavin therapy has been shown to increase corneal rigidity by 71.9% in porcine corneas and by 328.9% in human corneas.3
Purpose To analyze the efficacy of Corneal
Collagen Crosslinking with Riboflavin and Ultraviolet-A in progressive Keratoconus.Materials and Methods
This study was a nonrandomized, interventional, prospective trial which included 52 eyes of 45 patients who
were diagnosed to have progressive keratoconus. The study was conducted between January 2009 and June 2011 in the department of Ophthalmology, Little Flower Institute of Ophthalmology, Angamaly. An approval of the institutional ethics committee was taken prior to the beginning of the study. All the included patients provided written informed consent for the study.
Inclusion Criteria were documented progression of keratoconus by refraction (increase in cylinder by 1D or more over 1 year), or keratometry (increase in keratometry value of 1D or more over 1 year) with pachymetry more than 400 microns.4-6 Exclusion Criteria were corneal scar, pachymetry less than 400 microns, non-progressive keratoconus, ocular pathology other than keratectasia, especially cornea guttata or other
Keywords : keratoconus • crosslinking • riboflavin • ultraviolet a • spherical equivalent
Original Article
Seema KM DO, DNB
Cornea Consultant,Little Flower HospitalAngamaly, Cochin, Indiaemail id: [email protected]
*Address for correspondence
DOI: http://dx.doi.org/10.7869/djo.2013.4

24 Del J Ophthalmol 2013;24(1)
ISSN 0972-0200
endothelial irregularities, history of recurrent erosions, actual or intended pregnancy, not available for follow up examinations for 1 year and connective tissue disease.
A standardized form was completed for each patient documenting clinical findings including duration of symptoms, previous refraction, past treatment and predisposing ocular conditions. Pre collagen crosslinking work up included UCVA (uncorrected visual acuity), refraction and BCVA (best corrected visual acuity), slit lamp examination, keratometry, pachymetry, applanation tonometry and corneal topography. Patients using rigid contact lenses were asked not to wear them for at least 3 weeks before the preoperative examination and for 1 month after treatment.
Surgical Technique The central 7mm of the corneal epithelium was
removed using a blunt knife under topical anaesthesia with all aseptic precautions. Riboflavin 0.1% was used as photosensitizer. Riboflavin drops were applied every 5 minutes for 30 minutes. Then ultraviolet - A light of 370nm was applied for 30 minutes using 3 mW/cm2 irradiance. Even during this period riboflavin drops were applied every 5 minutes. After 30 minutes of irradiation, the ultraviolet source was removed. The eye was washed with saline. A bandage contact lens was fitted to the corneal surface until reepithelialisation.
Postoperatively patients were started on topical antibiotic, preservative free tear substitute, anti-inflammatory eye drops and oral analgesics. The patient was seen again on the first and third postoperative days. The bandage contact lens could be removed on the third postoperative day in most cases, once the epithelium healed. Further follow up visits were at 1week to rule out infection if any, 1month postoperatively and at 3, 6 and 12 months. Visual acuity, BCVA, keratometry, pachymetry and applanation tonometry ware recorded at each visit. Slit lamp examination was performed at each visit. Corneal topography was repeated at 12 months. To calculate the mean values and for comparisons, visual acuities were converted to the logMar scale.
Statistical AnalysisBased on the severity of the corneal curvature, the study
patients were categorized into 2 categories:a. category 1 - 47 - 52D in both meridians [22 eyes]b. category 2 - more than 52 in both meridians [30 eyes]
All calculations were performed with SPSS. Variables considered were best corrected visual acuity (BCVA), maximum keratometric reading in dioptres (max K), spherical equivalent in dioptres (SE), keratometric astigmatism (KA) and intraocular pressure by applanation tonometry (AT) at the pre-procedure visit and at 3,6 and 12 months after the procedure. Descriptives presented for these variables were the mean, standard deviation (SD), 95% confidence intervals (CI) etc. Further the data was plotted using techniques like error bars and box plots. A one factor
analysis of variance (ANOVA) was performed on the above variables.
Results
Of 52 eyes of 45 patients with progressive keratoconus were enrolled in this study, 69.2% were males and 30.8% were females; 28.8% were less than 18 years, 63.5% were between 18 and 30 years and 7.7% above 30 years. Forty patients (47 eyes) completed one year follow up. Five cases lost to follow up after six months. At presentation Vogt’s striae could be seen in 20 eyes. Epithelial healing was completed within a mean of 3.25 + 1.4 days in all the patients. At one month all eyes had stromal haze which disappeared by 3months.
Regarding BCVA an improvement of 1 or more lines on the Snellen’s chart was accepted as an improvement. Similarly a loss of one or more lines on the Snellen’s chart was accepted as worsening. The other cases were considered to be stable. In all cases BCVA dropped at the one month follow up visit, but stabilized or started improving by 3 months. The initial drop could be attributed to the stromal haze following the procedure. The stromal haze cleared completely at the 3rd month follow up visit in all patients.
An improvement of BCVA was seen in 42.31% of category 1 and 26.92% of category 2. An improvement of 2 lines was seen in 9 patients and an improvement of 1 line was seen in 15. BCVA was stable in 46.15% of category 1 and 60.39% of category 2. BCVA worsened in 11.54% of category1 and 12.69% of category 2.
Figure 1 depicts the error bars showing the progression of BCVA across time. The mean preoperative BCVA in category 1 is 0.136 with a standard deviation of 0.143. At the end of one year, the mean postoperative BCVA in this category is 0.057 with a standard deviation of 0.108. A one-way ANOVA confirms that the difference in means of the value before and after the procedure at 1 year does not differ significantly (p value 0.451). The mean preoperative BCVA in category 2 is 0.414 with a standard deviation of 0.183. At the end of 1 year, the mean BCVA in this group was 0.300 with a standard deviation of 0.205. A one way ANOVA again confirms that the means of the preoperative and postoperative BCVA values does not differ significantly (p value 0.486). Hence the procedure can be claimed to preserve the visual acuity.
Changes in the maximum K reading in dioptres was also analysed over 1 year. An increase of 1D or more in the max K reading was considered to be progression of the ectasia. A decrease of 1 D or more in the max K reading was considered to be regression. The ectasia was considered to be stable in those cases where the K value continued to be within K + / - 1D. Max k reading showed regression in 32% of category 1 and 36.36% of category 2. Mean keratometric values decreased by 1.2D in category 1 and 1.02D in category 2. It was found to be stable in 61.54% of category 1 and 54.54% of category 2. Max k worsened in 6.46% of category 1 and 9.09% of category2.
Figure 2 depicts the error bars showing the change in max K reading across time. The mean preoperative max K
Original Article Jabbar A, KM Seema
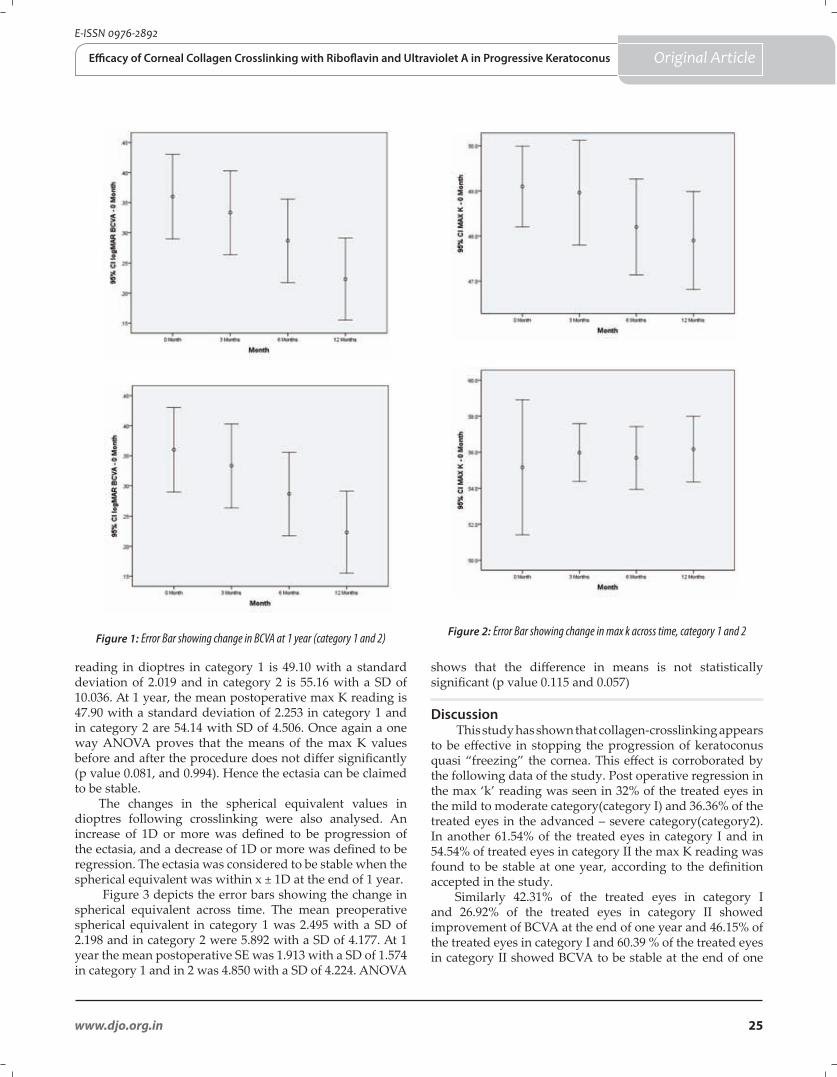
25www.djo.org.in
E-ISSN 0976-2892
Figure 1: Error Bar showing change in BCVA at 1 year (category 1 and 2)
reading in dioptres in category 1 is 49.10 with a standard deviation of 2.019 and in category 2 is 55.16 with a SD of 10.036. At 1 year, the mean postoperative max K reading is 47.90 with a standard deviation of 2.253 in category 1 and in category 2 are 54.14 with SD of 4.506. Once again a one way ANOVA proves that the means of the max K values before and after the procedure does not differ significantly (p value 0.081, and 0.994). Hence the ectasia can be claimed to be stable.
The changes in the spherical equivalent values in dioptres following crosslinking were also analysed. An increase of 1D or more was defined to be progression of the ectasia, and a decrease of 1D or more was defined to be regression. The ectasia was considered to be stable when the spherical equivalent was within x ± 1D at the end of 1 year.
Figure 3 depicts the error bars showing the change in spherical equivalent across time. The mean preoperative spherical equivalent in category 1 was 2.495 with a SD of 2.198 and in category 2 were 5.892 with a SD of 4.177. At 1 year the mean postoperative SE was 1.913 with a SD of 1.574 in category 1 and in 2 was 4.850 with a SD of 4.224. ANOVA
Original Article
Figure 2: Error Bar showing change in max k across time, category 1 and 2
Efficacy of Corneal Collagen Crosslinking with Riboflavin and Ultraviolet A in Progressive Keratoconus
shows that the difference in means is not statistically significant (p value 0.115 and 0.057)
Discussion
This study has shown that collagen-crosslinking appears to be effective in stopping the progression of keratoconus quasi “freezing” the cornea. This effect is corroborated by the following data of the study. Post operative regression in the max ‘k’ reading was seen in 32% of the treated eyes in the mild to moderate category(category I) and 36.36% of the treated eyes in the advanced – severe category(category2). In another 61.54% of the treated eyes in category I and in 54.54% of treated eyes in category II the max K reading was found to be stable at one year, according to the definition accepted in the study.
Similarly 42.31% of the treated eyes in category I and 26.92% of the treated eyes in category II showed improvement of BCVA at the end of one year and 46.15% of the treated eyes in category I and 60.39 % of the treated eyes in category II showed BCVA to be stable at the end of one
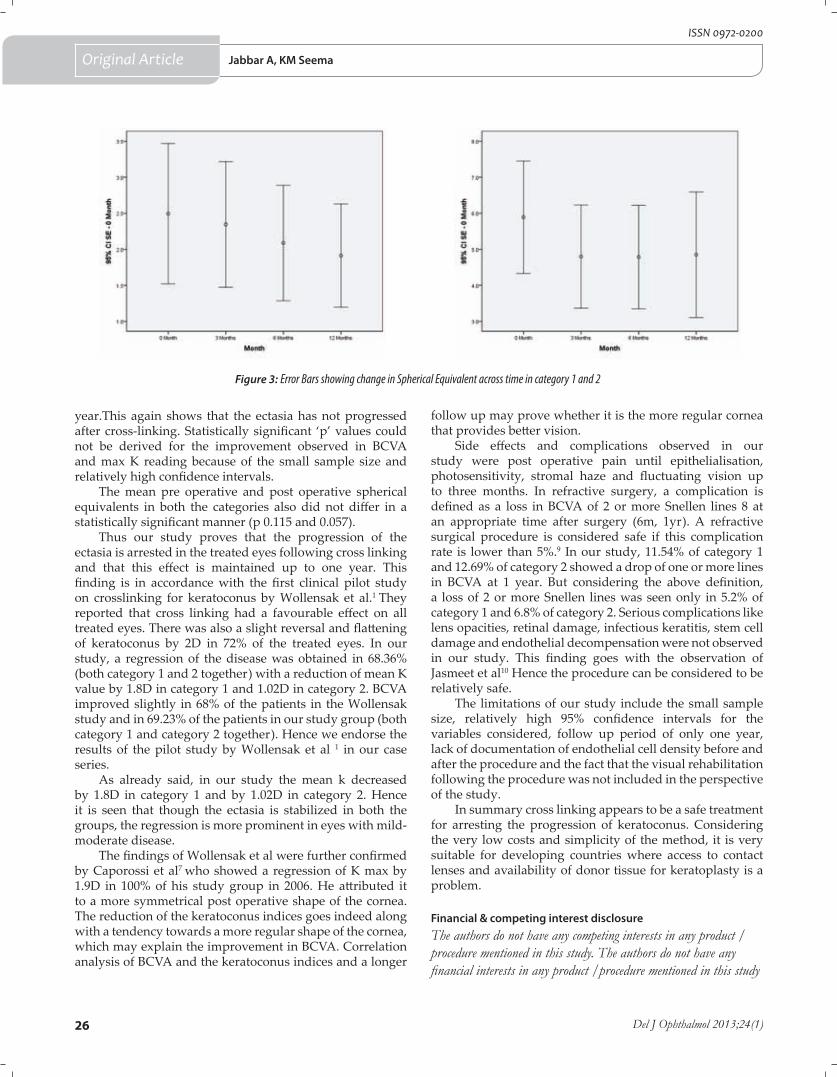
26 Del J Ophthalmol 2013;24(1)
ISSN 0972-0200
Original Article
year.This again shows that the ectasia has not progressed after cross-linking. Statistically significant ‘p’ values could not be derived for the improvement observed in BCVA and max K reading because of the small sample size and relatively high confidence intervals.
The mean pre operative and post operative spherical equivalents in both the categories also did not differ in a statistically significant manner (p 0.115 and 0.057).
Thus our study proves that the progression of the ectasia is arrested in the treated eyes following cross linking and that this effect is maintained up to one year. This finding is in accordance with the first clinical pilot study on crosslinking for keratoconus by Wollensak et al.1 They reported that cross linking had a favourable effect on all treated eyes. There was also a slight reversal and flattening of keratoconus by 2D in 72% of the treated eyes. In our study, a regression of the disease was obtained in 68.36% (both category 1 and 2 together) with a reduction of mean K value by 1.8D in category 1 and 1.02D in category 2. BCVA improved slightly in 68% of the patients in the Wollensak study and in 69.23% of the patients in our study group (both category 1 and category 2 together). Hence we endorse the results of the pilot study by Wollensak et al 1 in our case series.
As already said, in our study the mean k decreased by 1.8D in category 1 and by 1.02D in category 2. Hence it is seen that though the ectasia is stabilized in both the groups, the regression is more prominent in eyes with mild-moderate disease.
The findings of Wollensak et al were further confirmed by Caporossi et al7 who showed a regression of K max by 1.9D in 100% of his study group in 2006. He attributed it to a more symmetrical post operative shape of the cornea. The reduction of the keratoconus indices goes indeed along with a tendency towards a more regular shape of the cornea, which may explain the improvement in BCVA. Correlation analysis of BCVA and the keratoconus indices and a longer
Figure 3: Error Bars showing change in Spherical Equivalent across time in category 1 and 2
Jabbar A, KM Seema
follow up may prove whether it is the more regular cornea that provides better vision.
Side effects and complications observed in our study were post operative pain until epithelialisation, photosensitivity, stromal haze and fluctuating vision up to three months. In refractive surgery, a complication is defined as a loss in BCVA of 2 or more Snellen lines 8 at an appropriate time after surgery (6m, 1yr). A refractive surgical procedure is considered safe if this complication rate is lower than 5%.9 In our study, 11.54% of category 1 and 12.69% of category 2 showed a drop of one or more lines in BCVA at 1 year. But considering the above definition, a loss of 2 or more Snellen lines was seen only in 5.2% of category 1 and 6.8% of category 2. Serious complications like lens opacities, retinal damage, infectious keratitis, stem cell damage and endothelial decompensation were not observed in our study. This finding goes with the observation of Jasmeet et al10 Hence the procedure can be considered to be relatively safe.
The limitations of our study include the small sample size, relatively high 95% confidence intervals for the variables considered, follow up period of only one year, lack of documentation of endothelial cell density before and after the procedure and the fact that the visual rehabilitation following the procedure was not included in the perspective of the study.
In summary cross linking appears to be a safe treatment for arresting the progression of keratoconus. Considering the very low costs and simplicity of the method, it is very suitable for developing countries where access to contact lenses and availability of donor tissue for keratoplasty is a problem.
Financial & competing interest disclosureThe authors do not have any competing interests in any product / procedure mentioned in this study. The authors do not have any financial interests in any product /procedure mentioned in this study
27www.djo.org.in
E-ISSN 0976-2892
Original Article
References
1. Wollensak G, Spoerl E, Seiler T. Riboflavin/ ultraviolet – A induced cross linking for the treatment of keratoconus. Am. J Ophthalmol 2003; 135:62–7.
2. Wollensak G. Cross linking treatment of progressive keratoconus: New hope. Curr Opin ophthalmol 2006; 17:356 – 60.
3. Marcus Kohlhaas, Eberhard Spoerl. Biomechanical evidence of crosslinks in corneas after C3R. JCRS 2006; 32:279-83.
4. Raiskup-Wolf F, Hoyer A, Spoerl E, Pillunat LE. Collagen crosslinking with riboflavin and ultraviolet-A light in keratoconus: long-term results. J Cataract Refract Surg 2008 ; 34: 796-801.
5. Wittig-Silva, C; Whiting M, Lamoureux E, Lindsay RG, Sullivan LJ, Snibson GR. A Randomized Controlled Trial of Corneal Collagen Cross-linking in Progressive Keratoconus: Preliminary Results. Journal of Refractive Surgery. 2008: S720-5.
6. Hersh PS, Greenstein SA, Fry KL. Corneal collagen crosslinking for keratoconus and corneal ectasia: One-year results. J Cataract Refract Surgery 2011 ;149-160.
7. Caporossi A, Baiocchi S, Mazzotta C, et al. Parasurgical therapy for keratoconus by riboflavin – ultraviolet type A rays induced crosslinking of corneal collagen. J. Cataract Refract Surg 2006; 32:837-45.
8. U.S. Food and Drug Administration. Center for Devices and Radiological Health. Checklist of information usually submitted in an investigational device exemptions application for refractive surgery. www.fda.gov/cdrh/ode/2093.html.
9. Kanellopoulos AJ, Binder PS. Crosslinking with sequential topography guided PRK: a temporizing alternative for penetrating keratoplasty in keratoconus. Cornea 2007; 26:891-5
10. Jasmeet S. Dhaliwal,et al. Corneal collagen cross linking: A confocal, electron and light microscopy study of eye bank corneas. Cornea 2009; 28:62-7.
Efficacy of Corneal Collagen Crosslinking with Riboflavin and Ultraviolet A in Progressive Keratoconus
Postgraduates may send in their thesis work as ORIGINAL ARTICLES to the EDITOR–IN–CHIEF, Delhi Journal of Ophthalmology. Please specify that the submission is to be entered into the YOUNG OPHTHALMOLOGISTS section for consideration for best paper award. Please refer to the INFORMATION FOR AUTHORS section for further details.
Please write to [email protected] for any clarifications regarding submissions to Delhi Journal of Ophthalmology.
Dr M.VANATHI MDEditor-in-chief
Delhi Journal of Ophthalmology
Announcement
28 Del J Ophthalmol 2013;24(1)
ISSN 0972-0200
Original Article
Comparison of Visual Evoked Potential Components In Female Patients of Primary Open Angle Glaucoma with Age Matched Control FemalesDelhi J Ophthalmol 2013; 24 (1): 28-33
Objective: To compare the P100 latency and P100 amplitude of pattern reversal visual evoked potential VEP in a cohort of female patients having primary open angle glaucoma (POAG) with those of age matched control females.
Materials: This rural hospital based study was conducted in the Neurophysiology unit of the Department of Physiology of our institute. The study comprised of pattern reversal visual evoked potential (PRVEP) recordings from 244 eyes (92 POAG eyes and 152 control eyes).
Study Design: This was a comparative case- control study.
Methods: VEP recordings were performed with the stimulus configuration consisting of the transient pattern reversal method in which a black and white checker board was generated (full field) and displayed on VEP Monitor by an electronic pattern regenerator inbuilt in an Evoked Potential Recorder (RMS EMG EP MARK II, Recorders and Medicare Systems, Chandigarh). VEP waveform, latencies and amplitude were measured in all subjects.
Results: The mean age of POAG females (N=46) was 55 ± 10.50 years and the mean age of control females (N=76) was 54.30 ± 10.62 years. The age range for both the groups was 40-79 years. On comparison among all the age groups, the mean P100 latency of POAG patients was 98.13±6.39 msec and the mean P100 latency of the controls was 97.14 ± 4.46 msec. The mean amplitude of P100 in POAG patients was less than that of control subjects in the almost all the age groups. It was 4.48 ± 1.39 µV in POAG cases as compared to 6.20±2.02 µV in the controls of the age group 60-69 years and it was 3.76 ± 2.35 µV in POAG cases as compared to 4.36± 0.67µV in the controls of the age group 70-79 years.
Conclusion: Age wise and gender wise case control comparison of PRVEP components in our study subjects revealed that the eyes of females of POAG group have shown longer P100 latencies and produced diminished amplitude than the control eyes. The inter-eye difference of all the VEP parameters in the POAG group was significantly greater than those of controls. While in the control group, there was negligible inter-ocular difference between the two eyes of the same sex.
*Ruchi Kothari,**Pradeep Bokariya***Smita Singh, #Ramji Singh*Assistant Professor, Dept. of Physiology, **Assistant Professor Dept. of Anatomy, *** Professor, Dept. of Ophthalmology
Mahatma Gandhi Institute of Medical Sciences, Sevagram, Wardha – 442102, Maharashtra, India#Professor, Dept. of Physiology, AIIMS, Patna, Bihar, India
IntroductionPattern evoked visual responses have
become a reliable tool to recognize lesions in the optic pathway. Pattern Reversal Visual Evoked Potentials (PRVEPs) are characterized by an initial small negative (N70), followed by a major positive wave (P100) and then by a negative wave (N155). P100 is the hallmark of full field VEPs. It is the most consistent and least variable peak.1 It produces maximum excursion
when active electrode is placed at mid-occipital position.Gender is presumed to be one of the factors causing inter-individual variability in the brain’s visual electrophysiological parameters like VEP.2 Diminutive latency and greater amplitude of VEPs have been described in females as compared to males in some studies in the past.3-10 It is unclear whether these changes are related to the smaller anatomic size of head of females or to hormonal factors.
Keywords : open angle glaucoma • females • P100 latency • P100 amplitude
Ruchi Kothari M.Sc.(Medical) Physiology
Quarter No.1, MLK Colony,MGIMS & Kasturba Health Society Campus Sevagram,Wardha – 442102, Maharashtra, Indiaemail id: [email protected]
*Address for correspondence
DOI: http://dx.doi.org/10.7869/djo.2013.5

29www.djo.org.in
E-ISSN 0976-2892
Some very recent researches have reported that probably the gender based disparity in VEP components is due to the variations in head circumference.11,12 Some other attempts in recent years13,14 have also been made to explore the influence of gender on Pattern VEPs although their results have been inconsistent and in earlier reports3 the differences obtained between the two sexes were not significant.
Moreover, it is perceived that there is scarcity of data in literature related to changes in the VEPs with respect to gender especially in ocular diseases like glaucoma. We therefore conducted this study with an aim to investigate the variations of VEP components in a cohort of female glaucoma patients and a comparison was made with visual evoked responses of age matched control females.
Material and MethodsSettings & Design
Tertiary care rural hospital based case control studyThe patient group in this study consisted of 46 females diagnosed as having primary open angle glaucoma (POAG) by the ophthalmologist at the Glaucoma Clinic of Department of Ophthalmology. The age matched controls comprised of 76 healthy and normal female volunteers. All the subjects were selected after proper screening as per inclusion and exclusion criteria enumerated below. VEP investigation was performed in the Neurophysiology unit of the Department of Physiology of the institute. Both the eyes of two groups of the subjects had glaucoma and both were included in the study. Thus, Pattern Reversal VEP recordings from 244 eyes (92 POAG eyes and 152 control eyes) in total were obtained for the present study. Inclusion Criteria for controls
Control subjects were those having age > 40 years and < 79 years, Best-corrected visual acuity 6/6 (with or without corrective glasses), IOP <21 mmHg (as measured by the Non contact tonometer, Open angle at gonioscopy, Normal optic nerve head and retinal nerve fiber layer on clinical examination, Negative family history for glaucoma in a first degree relative, Normal pupillary size (2-4mm) and reactions, Normal Fundus and optic disc.
Inclusion Criteria for diagnosing POAG patients Open angle of normal appearance at gonioscopy, intra-
ocular pressure (IOP) more than 21 mmHg (as measured by the noncontact tonometer), characteristic glaucomatous optic nerve head changes, typical Glaucomatous visual field defects, IOP < 21 mm Hg for patients under pharmacological (medical) treatment. The remaining inclusion criteria were the same as that of controls. Glaucoma patients were either with or without treatment i.e. were recently diagnosed or already known cases on treatment.
Exclusion Criteria for POAG patientsVisual acuity (BCVA) <6/6, Ptosis/Strabismus/ Amblyopia,
Corneal or lenticular opacities, Retinitis pigmentosa, Multiple sclerosis (MS), Albinism, Diabetes mellitus, Hereditary disorders, Diseases involving macula, retina or visual pathway,
Optic neuritis, history of relevant neurological or heart disease or of drug abuse, past history of serious visual problems, recent eye medications (mydriatics or cycloplegics in the past 12 hours), Miotic pupil, High myopia, hypermetropia or astigmatism > 3 diopters, Parkinson’s disease, previous intraocular surgery except for uncomplicated cataract extraction, Secondary or angle closure glaucoma and any unco-operative subject or a subject with incomplete screening and examination was excluded from the study.
Exclusion Criteria for controls
The subjects having Glaucoma/Ocular Hypertension were excluded. All the other exclusion criteria were the same as for POAG patients.
The glaucoma group and control population was divided into 4 categories as -
Group I: consisting of subjects in the age range of 40-49 yearsGroup II: including subjects in the age range of 50-59 yearsGroup III: comprising of subjects in the age range of 60-69 yearsGroup IV: consisting of subjects in the age range of 70-79 years
Ethics consideration: Each subject gave informed consent to participate in this study. Ethics approval from the Institutional Ethics committee was obtained prior to the study.
Physical parameters:Height of the subject was measured in cms by using
standard anthropometric instruments in anatomical position. Head circumference (in cms) of the subject was measured
by using measuring tape in anatomical position.Pupil size was assessed with the help of a pupillometer
and was recorded in mm.Intra-ocular Pressure was recorded in mmHg by using
Non-contact tonometer.Measurements were carried out by a single person to eliminate the personal factor. A single expert ophthalmologist conducted a complete ophthalmic examination of each subject which included Visual acuity, Anterior Segment Examination, Posterior segment examination (Fundoscopy), and Automated Perimetry.
Methodology for VEPVEP recordings were done in accordance to the standardized
methodology of International Federation of Clinical Neurophysiology (IFCN) Committee Recommendations15 and International Society for Clinical Electrophysiology of Vision (ISCEV) Guidelines16 and montages were kept as per 10-20 International System of EEG Electrode placements.17 The stimulus configuration was transient pattern reversal method in which a black and white checker board was generated (full field) on a VEP Monitor by an Evoked Potential Recorder (RMS EMG EP MARK II). Each subject was seated comfortably at a distance of 1 meter away from the screen of the VEP monitor. A fixation point (red square) was positioned at a corner of four
Original ArticleVEP in POAG

30 Del J Ophthalmol 2013;24(1)
ISSN 0972-0200
checks which were located at the center of the field. The rate of pattern reversal was 1 Hz. The recording sensitivity was kept at 2μV. The electrode impedance was kept below 5KΩ. The sweep duration was maintained at 300 ms. Responses to 200 stimuli were amplified and averaged for each eye and two trials for each eye were obtained. The pattern stimulus luminance was 59 cd/sqm and the contrast was 80%. The signals recorded were filtered by low cut and high cut frequency filter through a band spread of 2-100 Hz.
Statistical analysis
The data obtained in the above recordings was statistically analysed using statistical programme SPSS software and computer programs using Microsoft excel software (Microsoft Corp, USA). One-way analysis of variance (ANOVA) test was used to compare the difference in latencies and amplitude duration between the controls and POAG eyes. Differences were considered to be significant at p< 0.05 and highly significant if p < 0.001.
ResultsSample characteristics
The mean age of POAG females (n=46) was 55 ± 10.50 years and the mean age of control females (n=76) was 54.30 ± 10.62 years. The age range for the subjects was 40 - 79 years. There was no statistically significant difference between the mean ages of both the groups. Hence the normal population and the glaucoma subjects were age matched for the analysis.
The mean height of POAG females was 151.04 ± 7.55 cm and the range of height was found to be from 130 - 165 cm. The mean height of controls was 150.21 ± 5.85 and the range of height was from 137 - 167 cm.
The mean head circumference of control females was 52.53 ± 1.42 cm and that of POAG females was 53.17 ± 1.51 cm. Among the females of POAG group and those of control group, the range of head circumference was the same and it was from 50 - 57 cm. The mean pupil size of 92 POAG female eyes was 2.66 ± 0.90 mm while that of 152 control eyes was 2.67 ± 0.69 mmHg. There was no statistically significant difference between the height, head circumference and pupil size among both the groups under study.
The mean intraocular pressure in females of POAG group was 14.71 ± 3.82 mmHg, while in control group, it was 12.88 ± 1.36 mmHg.
(Table 1) compares the mean ± SD of P100 latency in eyes of female patients of glaucoma group with that of females in control group. For the age groups 60 - 69 and 70 - 79 years, eyes of POAG females showed prolonged latencies in comparison with the control group. The difference was statistically significant in group IV. Overall gender wise comparison in all the age groups (figure 1) shows that mean P100 latency of eyes of females in glaucoma group (98.13 ± 6.39 msec) is prolonged than the mean P100 latency of eyes of control female group (97.14 ± 4.46 msec) although the difference was not statistically significant. The mean ± SD of the absolute latencies of the peak of positive wave P100 in each of the monocular recordings along
Original Article
with their inter-ocular differences that were recorded in females of the POAG patients in each group are shown in (Table 2). The mean ± SD of the absolute latencies of the peak of positive wave P100 in each of the monocular recordings along with their inter-ocular differences that were recorded in females among the controls in each group are shown in (Table 3). It is clear from the above table that there is negligible inter-ocular difference between the two eyes. However, the inter-eye difference of the VEP parameters in the POAG group was significantly greater than controls. The reason for this difference could be the severe glaucomatous damage in the one of the eyes having producing greater abnormality of VEP response as compared to the other which possessed mild to moderate glaucomatous changes. A significant correlation was obtained between P100 latency and the glaucomatous damage. In POAG females, the maximum P100 latency in right eyes was obtained in 70-79 year group and it was 120.05 msec. In left eyes, the maximum P100 latency was recorded in the age group of 70-79 years which was 118.24 msec. The largest inter-ocular difference in females was seen in group IV. On the other hand; in control females, the maximum P100 latency obtained in right eyes was 106.90 msec. In left eyes, the maximum P100 latency was recorded in the age group of 70-79 yrs which was 109.40 msec. (Table 4) compares the mean ± SD of P100 amplitude in females of glaucoma group with that of females in control group. The data enumerated in the above table shows that for the groups I, III and IV, the glaucoma females had reduced amplitude in comparison with the control group; the reduction in group III being a significant one. However, the females of the group II of POAG patients had significantly (p<0.05) larger P100 amplitude than that in controls of same age.
Overall comparison in all the age groups shows that P100 amplitude of females in glaucoma group is diminished than the control group but the difference of means is not statistically significant (figure 2). The mean ± SD of P100 amplitude in each of the monocular recordings along with their inter-ocular differences that were recorded in females among the POAG patients in each age group are shown in (Table 5). The data implies that smallest amplitude and largest inter-eye difference was found in the oldest age group i.e. in 70-79 years. The maximum value of P100 amplitude recorded for females was 13.58 μv in left eye of a patient in group II. The mean ± SD of P100 amplitude in each of the monocular recordings along with their inter-ocular differences that were recorded in females among the controls in each age group are shown in (Table 6). The data in the above table indicates that smallest amplitude was found in the oldest age group i.e. in 70-79 years. The maximum value of P100 amplitude recorded was 16.20 μv in right eye of a female in group II. This clearly implies that P100 wave produced larger excursions in females in the control group which is a finding similar to the POAG group.
DiscussionThe role of gender in POAG is controversial with several
studies18-20 showing no gender difference in disease prevalence and a few others21,22 proving that men were more likely than women to have OAG so there is disparity of opinions on gender predisposition in POAG. Although some age-controlled
Kothari et al
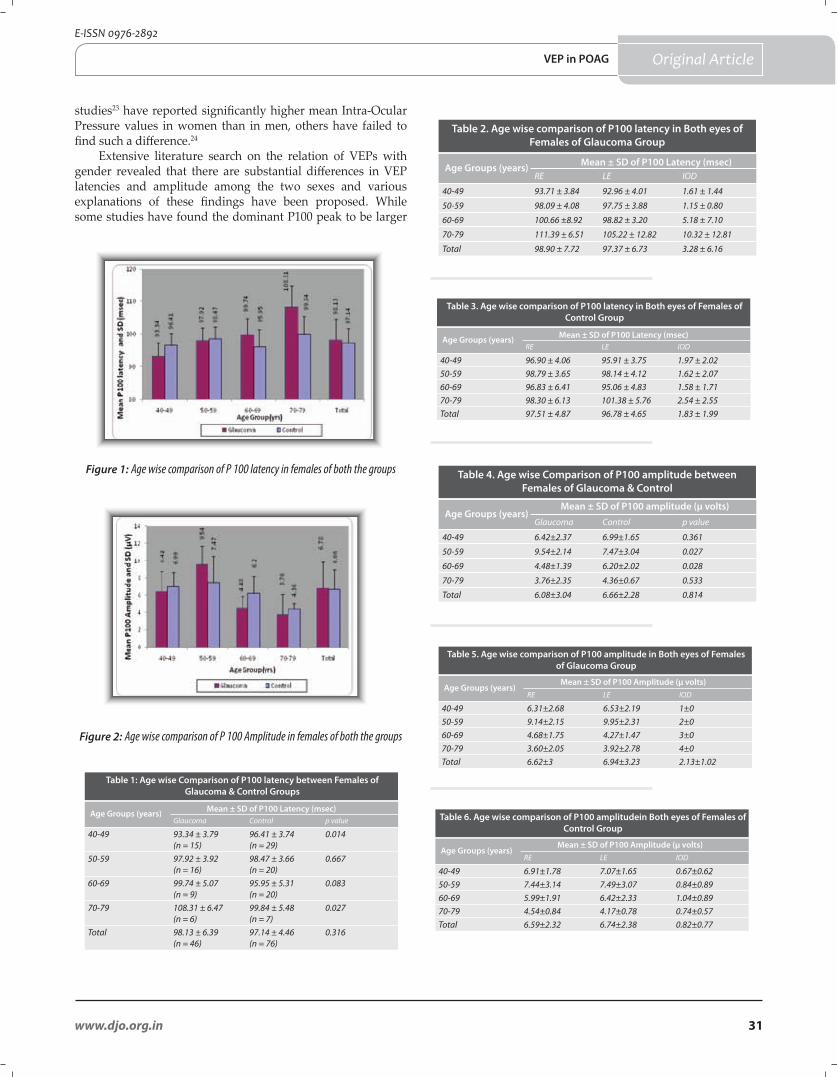
31www.djo.org.in
E-ISSN 0976-2892
studies23 have reported significantly higher mean Intra-Ocular Pressure values in women than in men, others have failed to find such a difference.24
Extensive literature search on the relation of VEPs with gender revealed that there are substantial differences in VEP latencies and amplitude among the two sexes and various explanations of these findings have been proposed. While some studies have found the dominant P100 peak to be larger
Original Article
Glaucoma Control p value
40-49 93.34 ± 3.79(n = 15)
96.41 ± 3.74(n = 29)
0.014
50-59 97.92 ± 3.92(n = 16)
98.47 ± 3.66(n = 20)
0.667
60-69 99.74 ± 5.07(n = 9)
95.95 ± 5.31(n = 20)
0.083
70-79 108.31 ± 6.47(n = 6)
99.84 ± 5.48(n = 7)
0.027
Total 98.13 ± 6.39(n = 46)
97.14 ± 4.46(n = 76)
0.316
Mean ± SD of P100 Latency (msec)Age Groups (years)
Table 1: Age wise Comparison of P100 latency between Females of Glaucoma & Control Groups
RE LE IOD
40-49 93.71 ± 3.84 92.96 ± 4.01 1.61 ± 1.44
50-59 98.09 ± 4.08 97.75 ± 3.88 1.15 ± 0.80
60-69 100.66 ±8.92 98.82 ± 3.20 5.18 ± 7.10
70-79 111.39 ± 6.51 105.22 ± 12.82 10.32 ± 12.81
Total 98.90 ± 7.72 97.37 ± 6.73 3.28 ± 6.16
Mean ± SD of P100 Latency (msec)Age Groups (years)
Table 2. Age wise comparison of P100 latency in Both eyes of Females of Glaucoma Group
RE LE IOD
40-49 96.90 ± 4.06 95.91 ± 3.75 1.97 ± 2.0250-59 98.79 ± 3.65 98.14 ± 4.12 1.62 ± 2.0760-69 96.83 ± 6.41 95.06 ± 4.83 1.58 ± 1.7170-79 98.30 ± 6.13 101.38 ± 5.76 2.54 ± 2.55Total 97.51 ± 4.87 96.78 ± 4.65 1.83 ± 1.99
Mean ± SD of P100 Latency (msec)Age Groups (years)
Table 3. Age wise comparison of P100 latency in Both eyes of Females of Control Group
RE LE IOD
40-49 6.31±2.68 6.53±2.19 1±050-59 9.14±2.15 9.95±2.31 2±060-69 4.68±1.75 4.27±1.47 3±070-79 3.60±2.05 3.92±2.78 4±0Total 6.62±3 6.94±3.23 2.13±1.02
Mean ± SD of P100 Amplitude (µ volts)Age Groups (years)
Table 5. Age wise comparison of P100 amplitude in Both eyes of Females of Glaucoma Group
Glaucoma Control p value
40-49 6.42±2.37 6.99±1.65 0.361
50-59 9.54±2.14 7.47±3.04 0.027
60-69 4.48±1.39 6.20±2.02 0.028
70-79 3.76±2.35 4.36±0.67 0.533
Total 6.08±3.04 6.66±2.28 0.814
Mean ± SD of P100 amplitude (µ volts)Age Groups (years)
Table 4. Age wise Comparison of P100 amplitude between Females of Glaucoma & Control
RE LE IOD
40-49 6.91±1.78 7.07±1.65 0.67±0.6250-59 7.44±3.14 7.49±3.07 0.84±0.8960-69 5.99±1.91 6.42±2.33 1.04±0.8970-79 4.54±0.84 4.17±0.78 0.74±0.57Total 6.59±2.32 6.74±2.38 0.82±0.77
Mean ± SD of P100 Amplitude (µ volts)Age Groups (years)
Table 6. Age wise comparison of P100 amplitudein Both eyes of Females of Control Group
Figure 1: Age wise comparison of P 100 latency in females of both the groups
Figure 2: Age wise comparison of P 100 Amplitude in females of both the groups
VEP in POAG

32 Del J Ophthalmol 2013;24(1)
ISSN 0972-0200
in females than males4,7,8,13 and many believe that this gender difference continues into adulthood7,10,13 other authors have found that Pattern VEP peak amplitude does not differ across gender.4,8 An analogous effect has also been reported for P100 peak latency, with some authors reporting shorter latencies in women5,11,13,14 and others reporting no gender difference.8,25 However we failed to obtain any reports of VEP alterations particularly in POAG females and their comparison to visually healthy females. This study investigated the variations of VEP components in female POAG patients and compared them with VEP responses of age matched control females.
As per age wise comparison of both the groups in females, the glaucoma females had reduced P100 amplitude in comparison with the control group for the groups I, III and IV. As a contrasting feature females of 50-59 years have shown significantly (p<0.05) larger P100 amplitude than that in controls of same age. This observation is in agreement with the evidence that PRVEP waves (N70-P100-N155) in older females are significantly larger than others and it was opined by La Marche et al9 that the visual system of older females is unusually responsive to patterned stimuli. However according to Dolman et al,26 in ages older than this group’s, the degenerative changes in the visual system which increase after the age of 60 may supersede the unusually larger VEP response. Larger amplitude of VEPs have been described in females by Dustman et al3, Synder et al4, La Marche et al9, Celesia et al10, Allison et al6. In our study also P100 wave produced larger excursions in females in both POAG group as well as the control group which is a finding similar to sex differences in peak-to-peak VEP amplitude obtained by Kaneda et al27 after eliminating effects of body height or age.
Females are typically documented to have 2 to 5 msec faster conduction velocity than age matched males by Kaufman.28 When control females were compared with glaucoma females, we found that P100 latency of females in glaucoma group was prolonged than the control group. The difference was statistically significant in females of youngest and oldest age groups.
A normal person loses almost 10,000 ganglion cells per year, and by the time they are 80 years of age, they will have lost 30 percent of their ganglion cells. In the case of open angle glaucoma, by the time vision loss becomes apparent, more than 50 percent of ganglion cells are destroyed. Out of these retinal ganglion cells that are lost over a 80- year life span, approximately half of those are responsible for macular function. Thus in glaucoma with progressive age, there is loss of neurons and degenerative changes occur in the striate cortex. Both of these reasons seem to be projected by the reduced P100 amplitude in the higher age group cases. This probably justifies the results obtained in the older POAG patients of the present study as compared to those of the younger age group in POAG.
ConclusionTo summarize, on evaluating the case control comparison,
eyes of females of POAG group demonstrated longer P100 latencies and decreased amplitude than the eyes of control females. Another notable finding which was unveiled in our
study on determining the Inter-ocular comparisons was that the inter-eye difference of all the VEP parameters in the POAG group was significantly greater than those of controls. While in the control group, there was negligible inter-ocular difference between the two eyes of the same sex.
It is now known that visual evoked response of males differs from that of females, so pooling their data would magnify the degree of inconsistency of their individual VEP parameters. Further it will also have a negative impact on the sensitivity of clinical evaluation of patients having ocular disorders especially glaucoma. From this study, we tried to evaluate the alteration of processing of the visual information along the visual pathway in open angle glaucoma by performing VEPs in POAG females as well as in control females. We found statistically significant difference in the form of prolongation of P100 latency and reduction of P100 amplitude accompanied by large inter-ocular differences in the POAG cases as compared to controls which should be taken into account while assessing the visual electrophysiological status of female subjects.
Financial & competing interest disclosureThe authors do not have any competing interests in any product/
procedure mentioned in this study. The authors do not have any financial interests in any product / procedure mentioned in this study
Original Article
References
1. Aminoff MJ, Goodin DS. Visual evoked potentials. J Clin Neurophysiol 1994; 11:493-9
2. Langrová J, Kremláček J, Kuba M, Kubová Z, Szanyi J. Gender Impact on Electrophysiological Activity of the Brain. Physiol Res 2012;61 (Suppl. 2): S119-S127.
3. Dustman RE, Beck EC. The effects of maturation and aging on the waveform of visually evoked potentials. Electroencephalogr Clin Neurophysiol 1969; 26:2-11.
4. Synder EW, Dustman RE, Shearer. Pattern reversal evoked potential amplitudes: Life span changes. Electroencephalogr Clin Neurophysiol 1981; 52:429-434.
5. Fenwick PB, Brown D, Hennesey J. The visual evoked response to pattern reversal in ‘normal’ 6-11-year-old children. Electroencephalogr Clin Neurophysiol 1981;51:49-62.
6. Allison T, Wood CC, Goff WR. Brainstem auditory, pattern reversal visual and short term somatosensory evoked potentials, latencies in relation to age, sex and brain and body size. Electroencephalogr Clin Neurophysiol 1983; 55:619-36.
7. Allison T, Hume AL, Wood CC, Goff WR. Developmental and aging changes in somatosensory, auditory and visual evoked potentials. Electroencephalogr Clin Neurophysiol 1984;58:14-24.
8. Cohn NB, Kircher J, Emmerson RY, Dustman RE. Pattern reversal evoked potentials: age, sex and hemispheric asymmetry. Electroencephalogr Clin Neurophysiol 1985; 62:399-405.
9. La Marche JA, Dobson WR, Cohn NB, Dustman RE. Amplitudes of visually evoked potentials to patterned stimuli: age and sex comparisons. Electroencephalogr Clin Neurophysiol 1986; 65:81-5.
10. Celesia GG, Kaufman D, Cone S. Effects of age and sex on pattern electroretinograms and visual evoked potentials. Electroencephalogr Clin Neurophysiol 1987;68:171.
11. Gregori B, Pro S, Bombelli F, La Riccia M, Accornero N. VEP latency: sex and head size. Clin Neurophysiol. 2006;117: 1154-7
12. Kothari R, Singh R, Singh S, Bokariya P. Effect of head
Kothari et al

33www.djo.org.in
E-ISSN 0976-2892
Original Article
circumference on parameters of pattern reversal VEP in healthy adults of central India. Nepal Med Coll J. 2012; 14:75-9.
13. Emmerson-Hanover R, Shearer DE, Creel DJ, Dustman RE. Pattern reversal evoked potentials: gender differences and age-related changes in amplitude and latency. Electroencephalogr Clin Neurophysiol 1994; 92:93-101.
14. Malcolm CA, McCulloch DL, Shepherd AJ. Pattern-reversal visual evoked potentials in infants: gender differences during early visual maturation. Dev Med Child Neurol 2002; 44:345-51.
15. Celesia GG, Bodis-Wollner I, Chatrian GE, Harding GFA, Sokol S, Spekreijse H. Recommended standards for electroretinograms and visual evoked potentials. Report of an International Federation of Clinical Neurophysiology (IFCN) Committee. Electroencephalogr Clin Neurophysiol 1993; 87:421-36
16. Odom VJ, Bach M, Brigell M, Holder GE, McCulloch DA, Tormene AP, Vaegan. ISCEV standard for clinical visual evoked potentials (2009 update) Doc Ophthalmol 2010; 120:111-9.
17. American Clinical Neurophysiology Society. Guideline 5: guidelines for standard electrode position nomenclature. J Clin Neurophysiol 2006; 23:107–10.
18. Javeitt JC, McBean AM, Nicholson GA, Babish JD, Warren JL, Krakauer H. Undertreatment of among Black Americans. N Engl J Med 1991; 325:1418-22.
19. Wilensky JT, Gandhi N, Pan T. Racial influences in open-angle glaucoma. Ann Ophthalmol 1978; 10:1398-402.
20. Coulehan JL, Helzlsouer KJ, Rogers KD, Brown SI. Racial differences in intraocular tension and glaucoma surgery. Am J Epidemiol 1980; 111:759-68.
21. Rotchford AP, Johnson GJ. Glaucoma in Zulus: a population-based cross-sectional survey in a rural district in South Africa. Arch Ophthalmol 2002; 120:471-8.
22. Sommer A, Tielsch JM, Katz J, Quigley HA, Gottsch JD, Javitt JC, Martone JF, Royall RM, Witt KA, Ezrine S. Racial differences in the cause-specific prevalence of blindness in east Baltimore. N Engl J Med 1991; 325:1412-7.
23. Mason RP, Kosoko O, Wilson MR, Martone JF, Cowan CL Jr, Gear JC, Ross-Degnan D. National survey of the prevalence and risk factors of glaucoma in St. Lucia, West Indies. Part I. Prevalence findings. Ophthalmology 1989; 96:1363-8.
24. Teilsch JM, Sommer A, Katz J, et al. Racial variations in the prevalence of primary open-angle glaucoma: the Baltimore Eye Survey. JAMA 1991; 266:369–74.
25. Mitchell KW, Howe JW, Spencer SR. Visual evoked potentials in the older population: age and gender effects. Clin Phys Physiol Meas 1987; 8:317-24.
26. Dolman CL, McCormick AQ, Drance SM. Aging of the optic nerve. Arch Ophthalmol 1980; 98:205.
27. Kaneda Y, Nakayama H, Kagawa K, Furuta N, Ikuta T. Sex differences in visual evoked potential and electroencephalogram of healthy adults. Tokushima J Exp Med 1996; 43:143-57.
28. Kaufman DI. Ancillary Electrophysiologic Testing in: Neuro-Ophthalmology – the Practical Guide. Leonard A. Levin Anthony C. Arnold (Eds). Thieme Medical Publishers, New York, 2005: 424
VEP in POAG
National Eye Donation FortnightAugust 25 – September 8, 2013
Spread information about Eye Donation and motivate others to help this cause
Come forward with all your family members, relatives and friends to join this movement
Please consent to donate eyes of your deceased relative
Contact the nearest Eye Bank for information regarding pledge forms
www.rpcos.org/pledge
NATIONAL EYE BANK
Prof Radhika TandonOffice In charge National Eye Bank Dr R P Centre, AIIMS, New Delhi
Prof R V AZADChief - Dr R P Centre
AIIMS, New Delhi
34 Del J Ophthalmol 2013;24(1)
ISSN 0972-0200
Ocular Dirofilaria repens: not rare Delhi J Ophthalmol 2013; 24 (1): 34-36
Aim: To report three cases of ocular Dirofilaria repens.
Methods: Three patients, who presented to us with mass in preseptal and orbital region, and were not improving with parenteral and oral steroids, were investigated. Excisional biopsy of the mass was done and histopathological report was studied and reported.
Results: Histopathalogical examination revealed the mass to be degenerating filarial worms with surrounding inflammation.
Discussion: Dirofilaria repens is a filarial nematode that affects dogs and other carnivores. Infections in humans usually manifests as a single subcutaneous nodule, which is caused by a macrofilaria that is trapped by the immune system. Over past one decade dirofilaria repens has been reported in ocular tissues by many authors in India and abroad. We here with present three such cases, who presented to us in short span of time, indicating that this presentation is no more rare.
*Usha Kim, *#Mohit Gupta, *N. Vidhya, **Shanti*Department of orbit, oculoplasty &oncology,** PathologyAravind Eye Hospital, Madurai. India
*# Dr Omprakash Eye Institute, Amritsar, India
*Address for correspondence
Introduction Dirofilaria repens is a filarial nematode
that affects dogs and other carnivores such as cats, wolves, foxes, muskrats and sea lions. Although humans may become infected as aberrant hosts, the worms fail to reach adulthood while residing in a human body.
The life cycle of Diroflaria repens consists of five larval stages in a vertebral host and an arthropod (mosquito) intermediate host and vector. In the first stage, mated adult female worms produce thousands of microfilariae (larvae) into the circulation daily, which are ingested by mosquitoes in a blood meal. Larvae develop into infective larvae within the mosquito over the next 10–16 days, depending on environmental conditions, before being reintroduced back into a new host. Microfilariae undergo secondary developmental changes in the insect. For the final two stages of development, third-stage larvae are inoculated back into a vertebral host during an act of feeding. The adults of D. repens reside in the subcutaneous tissues of dogs and cats for the next several months before migrating to the heart, where they mature in 6–7 months. Adult worms are 1–2 mm in diameter (females are 25–30 cm in length, the males being shorter).1
Humans are accidental hosts because adult worms can not reach maturity in the heart or in the skin. Most infective larvae
introduced into humans are thought to be dying; therefore, infected individuals usually are not microfilaremic. Human disease is amicrofilaremic.
Infections in humans usually manifests as a single subcutaneous nodule, which is caused by a macrofilaria that is trapped by the immune system. Subcutaneous migration of the worm may result in local swellings with changing localization. In addition, rare cases of organ manifestation have been reported, affecting the lung, male genitals, female breast or the eye. The latter is found in particular during the migratory phase of the parasite.
Final diagnosis is established by microscopic examination of the excised worm. Making a definite species diagnosis on morphologic grounds is difficult, because a large number of zoonotic Dirofilaria species have been described that share morphologic features with D. repens.
Antifilarial medication for infected humans generally is not supported in the medical literature. One group of authors has recommended a single dose of Ivermectin followed by 3 doses of diethylcarbamazine (DEC) if the syndrome is recognized prior to surgery. However, most cases are diagnosed retrospectively, when histopathological sections of biopsy or excision material are viewed. In term
Keywords : dirofilaria • filaria • nematode
Mohit Gupta MS
Oculoplasty consultantDr Omprakash Eye Institute, Amritsar, Indiaemail: [email protected]
Case Report
DOI: http://dx.doi.org/10.7869/djo.2013.6

35www.djo.org.in
E-ISSN 0976-2892
of surgical care, excision of lesions and affected areas is the treatment of choice for patients with human dirofilariasis.
Over past one decade dirofilaria repens has been reported in ocular tissues by many authors in India and abroad. The worm has been reported in periocular tissues, subconjunctival space and anterior chamber (Table 1).
Case Series: Ocular Filariasis Case 1 – 74 yr old male patient, a known case of primary
open angle glaucoma, came with the complaints of painless progressive swelling in right eye for one month. On examination, his best corrected visual acuity was 6/6 in both eyes. He had right upper lid edema and a firm mass in pre septal region. Anterior and posterior segments of both eyes were normal with both eyes pseudophakia. Ocular movements were full. CT scan revealed preseptal cellulitis with soft tissue edema. Patient was given a course of parenteral steroid but showed only minimal improvement. Incisional biopsy was done and histopathology made a diagnosis of chronic granulomatous inflammation with degenerated filarial worm. Definitive species of worm could not be diagnosed as the worm was degenerating.
Case 2 – 42yr old female patient came with the complaints of painless progressive swelling in right lower lid for three weeks (Figure 1). On examination her unaided visual acuity on Snellens was 6/6 in both eyes. She had right lower lid edema and a firm mass in inferior orbital region with superior dystopia. Anterior and posterior segments of both eyes were normal. Ocular movements were full. CT scan revealed heterogeneously enhancing soft tissue lesion involving inferior quadrant of
Case Report
S.No. Authors Year Site
1. Chopra R, Bhatti SM, Mohan S, Taneja N4 2012 Anterior chamber
2. Joseph K, Vinayakumar AR, Criton S, Vishnu MS, Pariyaram SE.5 2011 Periorbital mass
3. Nath R, Gogoi R, Bordoloi N, Gogoi T.6 2010 Periorbital and subconjunctival cysts
4. Singh R, Shwetha JV, Samantaray JC, Bando G7 2010 Subcutaneous orbital mass
5. Tavakolizadeh S, Mobedi I Korean.8 2009 Orbital
6. Khechine-Martinez R, Doucet C, Blanchard S, Rouland JF, Labalette P.9 2009 Subconjuntival
7. Shenoi SD, Kumar P, Johnston SP, Khadilkar UN10 2009 Eyelid swelling
8. Fodor E, Fok E, Maka E, Lukáts O, Tóth J.11 2009 Subconjuntival
9. Eccher A, Dalfior D, Gobbo S, Martignoni G, Brunelli M, Decaminada W, Bonetti F, Rivasi F, Barbareschi M, Menestrina F. 12
2008 Subcutaneous orbital mass
10. Beden U, Hokelek M, Acici M, Umur S, Gungor I, Sullu Y.13 2007 Inferior orbital rim
11. Sathyan P, Manikandan P, Bhaskar M, Padma S, Singh G, Appalaraju B.14 2006 Sub tenons
12. Mahesh G, Giridhar A, Biswas J, Saikumar SJ, Bhat A.15 2005 Lid tumor
13. Ittyerah TP, Mallik D16 2004 Subcutaneous
14. Gautam V, Rustagi IM, Singh S, Arora DR17 2002 Subconjuntival
15. Nadgir S, Tallur SS, Mangoli V, Halesh LH, Krishna BV18 2001 Subconjuntival
16. Sekhar HS, Srinivasa H, Batru RR, Mathai E, Shariff S, Macaden RS19 2000 Eyelid
Table 1: Reported sites of ocular Dirofilaria infection
Figure 1: Pre operative with mass in lower lid and infra orbital region
right orbit and preseptal region (figure 2). Excisional biopsy was done and histopathology made a diagnosis of chronic granulomatous inflammation with partially degenerated filarial nematode (Figure 3). Post operative period was uneventful and on last follow up visit on 2 months, she had no evidence of mass (Figure 4).
Case 3 – 47yr old female came with the complaints of painless progressive swelling in left upper lid for one month. On examination her unaided visual acuity on snellens was 6/12 in both eyes. She had left upper lid edema and a firm mass in supraorbital region. Anterior and posterior segments of both eyes were normal with both eyes early immature cataract. Ocular movements were full. CT scan revealed orbital preseptal soft tissue swelling with left supra orbital soft tissue edema. Excisional biopsy was done and histopathology made a diagnosis of chronic granulomatous inflammation with partially degenerated filarial nematode. Patient was asymptomatic on follow up visits.
Ocular Dirofilaria repens: not rare
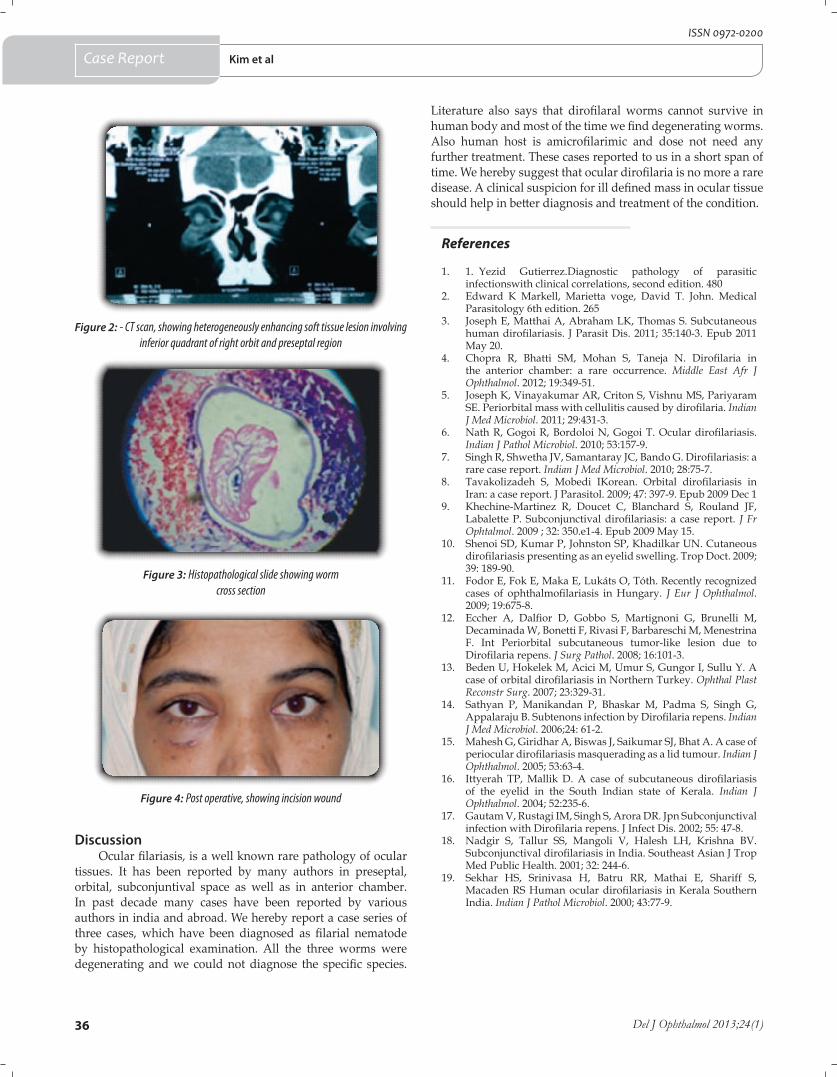
36 Del J Ophthalmol 2013;24(1)
ISSN 0972-0200
Figure 2: - CT scan, showing heterogeneously enhancing soft tissue lesion involving inferior quadrant of right orbit and preseptal region
Case Report
Figure 3: Histopathological slide showing worm cross section
Figure 4: Post operative, showing incision wound
DiscussionOcular filariasis, is a well known rare pathology of ocular
tissues. It has been reported by many authors in preseptal, orbital, subconjuntival space as well as in anterior chamber. In past decade many cases have been reported by various authors in india and abroad. We hereby report a case series of three cases, which have been diagnosed as filarial nematode by histopathological examination. All the three worms were degenerating and we could not diagnose the specific species.
References
1. 1. Yezid Gutierrez.Diagnostic pathology of parasitic infectionswith clinical correlations, second edition. 480
2. Edward K Markell, Marietta voge, David T. John. Medical Parasitology 6th edition. 265
3. Joseph E, Matthai A, Abraham LK, Thomas S. Subcutaneous human dirofilariasis. J Parasit Dis. 2011; 35:140-3. Epub 2011 May 20.
4. Chopra R, Bhatti SM, Mohan S, Taneja N. Dirofilaria in the anterior chamber: a rare occurrence. Middle East Afr J Ophthalmol. 2012; 19:349-51.
5. Joseph K, Vinayakumar AR, Criton S, Vishnu MS, Pariyaram SE. Periorbital mass with cellulitis caused by dirofilaria. Indian J Med Microbiol. 2011; 29:431-3.
6. Nath R, Gogoi R, Bordoloi N, Gogoi T. Ocular dirofilariasis. Indian J Pathol Microbiol. 2010; 53:157-9.
7. Singh R, Shwetha JV, Samantaray JC, Bando G. Dirofilariasis: a rare case report. Indian J Med Microbiol. 2010; 28:75-7.
8. Tavakolizadeh S, Mobedi IKorean. Orbital dirofilariasis in Iran: a case report. J Parasitol. 2009; 47: 397-9. Epub 2009 Dec 1
9. Khechine-Martinez R, Doucet C, Blanchard S, Rouland JF, Labalette P. Subconjunctival dirofilariasis: a case report. J Fr Ophtalmol. 2009 ; 32: 350.e1-4. Epub 2009 May 15.
10. Shenoi SD, Kumar P, Johnston SP, Khadilkar UN. Cutaneous dirofilariasis presenting as an eyelid swelling. Trop Doct. 2009; 39: 189-90.
11. Fodor E, Fok E, Maka E, Lukáts O, Tóth. Recently recognized cases of ophthalmofilariasis in Hungary. J Eur J Ophthalmol. 2009; 19:675-8.
12. Eccher A, Dalfior D, Gobbo S, Martignoni G, Brunelli M, Decaminada W, Bonetti F, Rivasi F, Barbareschi M, Menestrina F. Int Periorbital subcutaneous tumor-like lesion due to Dirofilaria repens. J Surg Pathol. 2008; 16:101-3.
13. Beden U, Hokelek M, Acici M, Umur S, Gungor I, Sullu Y. A case of orbital dirofilariasis in Northern Turkey. Ophthal Plast Reconstr Surg. 2007; 23:329-31.
14. Sathyan P, Manikandan P, Bhaskar M, Padma S, Singh G, Appalaraju B. Subtenons infection by Dirofilaria repens. Indian J Med Microbiol. 2006;24: 61-2.
15. Mahesh G, Giridhar A, Biswas J, Saikumar SJ, Bhat A. A case of periocular dirofilariasis masquerading as a lid tumour. Indian J Ophthalmol. 2005; 53:63-4.
16. Ittyerah TP, Mallik D. A case of subcutaneous dirofilariasis of the eyelid in the South Indian state of Kerala. Indian J Ophthalmol. 2004; 52:235-6.
17. Gautam V, Rustagi IM, Singh S, Arora DR. Jpn Subconjunctival infection with Dirofilaria repens. J Infect Dis. 2002; 55: 47-8.
18. Nadgir S, Tallur SS, Mangoli V, Halesh LH, Krishna BV. Subconjunctival dirofilariasis in India. Southeast Asian J Trop Med Public Health. 2001; 32: 244-6.
19. Sekhar HS, Srinivasa H, Batru RR, Mathai E, Shariff S, Macaden RS Human ocular dirofilariasis in Kerala Southern India. Indian J Pathol Microbiol. 2000; 43:77-9.
Literature also says that dirofilaral worms cannot survive in human body and most of the time we find degenerating worms. Also human host is amicrofilarimic and dose not need any further treatment. These cases reported to us in a short span of time. We hereby suggest that ocular dirofilaria is no more a rare disease. A clinical suspicion for ill defined mass in ocular tissue should help in better diagnosis and treatment of the condition.
Kim et al
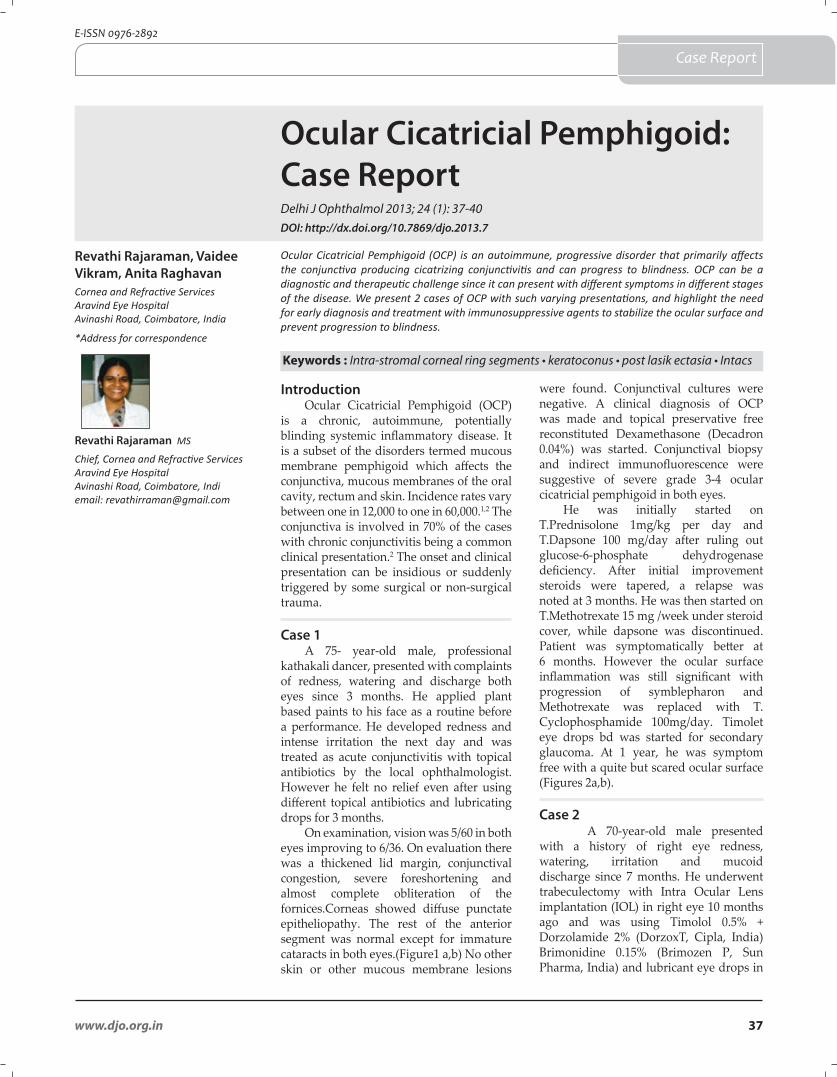
37www.djo.org.in
E-ISSN 0976-2892
Ocular Cicatricial Pemphigoid: Case ReportDelhi J Ophthalmol 2013; 24 (1): 37-40
Ocular Cicatricial Pemphigoid (OCP) is an autoimmune, progressive disorder that primarily affects the conjunctiva producing cicatrizing conjunctivitis and can progress to blindness. OCP can be a diagnostic and therapeutic challenge since it can present with different symptoms in different stages of the disease. We present 2 cases of OCP with such varying presentations, and highlight the need for early diagnosis and treatment with immunosuppressive agents to stabilize the ocular surface and prevent progression to blindness.
Revathi Rajaraman, Vaidee Vikram, Anita RaghavanCornea and Refractive ServicesAravind Eye HospitalAvinashi Road, Coimbatore, India
*Address for correspondence
IntroductionOcular Cicatricial Pemphigoid (OCP)
is a chronic, autoimmune, potentially blinding systemic inflammatory disease. It is a subset of the disorders termed mucous membrane pemphigoid which affects the conjunctiva, mucous membranes of the oral cavity, rectum and skin. Incidence rates vary between one in 12,000 to one in 60,000.1,2 The conjunctiva is involved in 70% of the cases with chronic conjunctivitis being a common clinical presentation.2 The onset and clinical presentation can be insidious or suddenly triggered by some surgical or non-surgical trauma.
Case 1
A 75- year-old male, professional kathakali dancer, presented with complaints of redness, watering and discharge both eyes since 3 months. He applied plant based paints to his face as a routine before a performance. He developed redness and intense irritation the next day and was treated as acute conjunctivitis with topical antibiotics by the local ophthalmologist. However he felt no relief even after using different topical antibiotics and lubricating drops for 3 months.
On examination, vision was 5/60 in both eyes improving to 6/36. On evaluation there was a thickened lid margin, conjunctival congestion, severe foreshortening and almost complete obliteration of the fornices.Corneas showed diffuse punctate epitheliopathy. The rest of the anterior segment was normal except for immature cataracts in both eyes.(Figure1 a,b) No other skin or other mucous membrane lesions
were found. Conjunctival cultures were negative. A clinical diagnosis of OCP was made and topical preservative free reconstituted Dexamethasone (Decadron 0.04%) was started. Conjunctival biopsy and indirect immunofluorescence were suggestive of severe grade 3-4 ocular cicatricial pemphigoid in both eyes.
He was initially started on T.Prednisolone 1mg/kg per day and T.Dapsone 100 mg/day after ruling out glucose-6-phosphate dehydrogenase deficiency. After initial improvement steroids were tapered, a relapse was noted at 3 months. He was then started on T.Methotrexate 15 mg /week under steroid cover, while dapsone was discontinued. Patient was symptomatically better at 6 months. However the ocular surface inflammation was still significant with progression of symblepharon and Methotrexate was replaced with T. Cyclophosphamide 100mg/day. Timolet eye drops bd was started for secondary glaucoma. At 1 year, he was symptom free with a quite but scared ocular surface (Figures 2a,b).
Case 2
A 70-year-old male presented with a history of right eye redness, watering, irritation and mucoid discharge since 7 months. He underwent trabeculectomy with Intra Ocular Lens implantation (IOL) in right eye 10 months ago and was using Timolol 0.5% + Dorzolamide 2% (DorzoxT, Cipla, India) Brimonidine 0.15% (Brimozen P, Sun Pharma, India) and lubricant eye drops in
Keywords : Intra-stromal corneal ring segments • keratoconus • post lasik ectasia • Intacs
Revathi Rajaraman MS
Chief, Cornea and Refractive ServicesAravind Eye HospitalAvinashi Road, Coimbatore, Indiemail: [email protected]
Case Report
DOI: http://dx.doi.org/10.7869/djo.2013.7
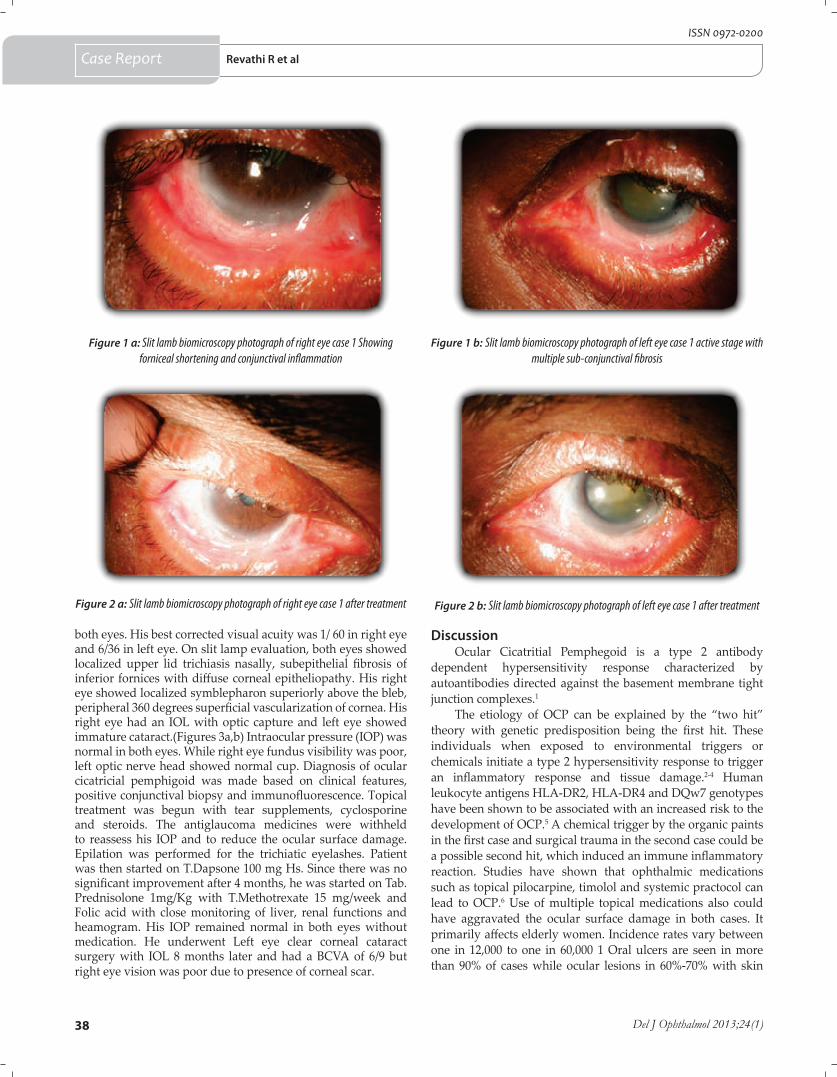
38 Del J Ophthalmol 2013;24(1)
ISSN 0972-0200
both eyes. His best corrected visual acuity was 1/ 60 in right eye and 6/36 in left eye. On slit lamp evaluation, both eyes showed localized upper lid trichiasis nasally, subepithelial fibrosis of inferior fornices with diffuse corneal epitheliopathy. His right eye showed localized symblepharon superiorly above the bleb, peripheral 360 degrees superficial vascularization of cornea. His right eye had an IOL with optic capture and left eye showed immature cataract.(Figures 3a,b) Intraocular pressure (IOP) was normal in both eyes. While right eye fundus visibility was poor, left optic nerve head showed normal cup. Diagnosis of ocular cicatricial pemphigoid was made based on clinical features, positive conjunctival biopsy and immunofluorescence. Topical treatment was begun with tear supplements, cyclosporine and steroids. The antiglaucoma medicines were withheld to reassess his IOP and to reduce the ocular surface damage. Epilation was performed for the trichiatic eyelashes. Patient was then started on T.Dapsone 100 mg Hs. Since there was no significant improvement after 4 months, he was started on Tab.Prednisolone 1mg/Kg with T.Methotrexate 15 mg/week and Folic acid with close monitoring of liver, renal functions and heamogram. His IOP remained normal in both eyes without medication. He underwent Left eye clear corneal cataract surgery with IOL 8 months later and had a BCVA of 6/9 but right eye vision was poor due to presence of corneal scar.
DiscussionOcular Cicatritial Pemphegoid is a type 2 antibody
dependent hypersensitivity response characterized by autoantibodies directed against the basement membrane tight junction complexes.1
The etiology of OCP can be explained by the “two hit” theory with genetic predisposition being the first hit. These individuals when exposed to environmental triggers or chemicals initiate a type 2 hypersensitivity response to trigger an inflammatory response and tissue damage.2-4 Human leukocyte antigens HLA-DR2, HLA-DR4 and DQw7 genotypes have been shown to be associated with an increased risk to the development of OCP.5 A chemical trigger by the organic paints in the first case and surgical trauma in the second case could be a possible second hit, which induced an immune inflammatory reaction. Studies have shown that ophthalmic medications such as topical pilocarpine, timolol and systemic practocol can lead to OCP.6 Use of multiple topical medications also could have aggravated the ocular surface damage in both cases. It primarily affects elderly women. Incidence rates vary between one in 12,000 to one in 60,000 1 Oral ulcers are seen in more than 90% of cases while ocular lesions in 60%-70% with skin
Figure 1 b: Slit lamb biomicroscopy photograph of left eye case 1 active stage with multiple sub-conjunctival fibrosis
Figure 1 a: Slit lamb biomicroscopy photograph of right eye case 1 Showing forniceal shortening and conjunctival inflammation
Figure 2 b: Slit lamb biomicroscopy photograph of left eye case 1 after treatmentFigure 2 a: Slit lamb biomicroscopy photograph of right eye case 1 after treatment
Case Report Revathi R et al
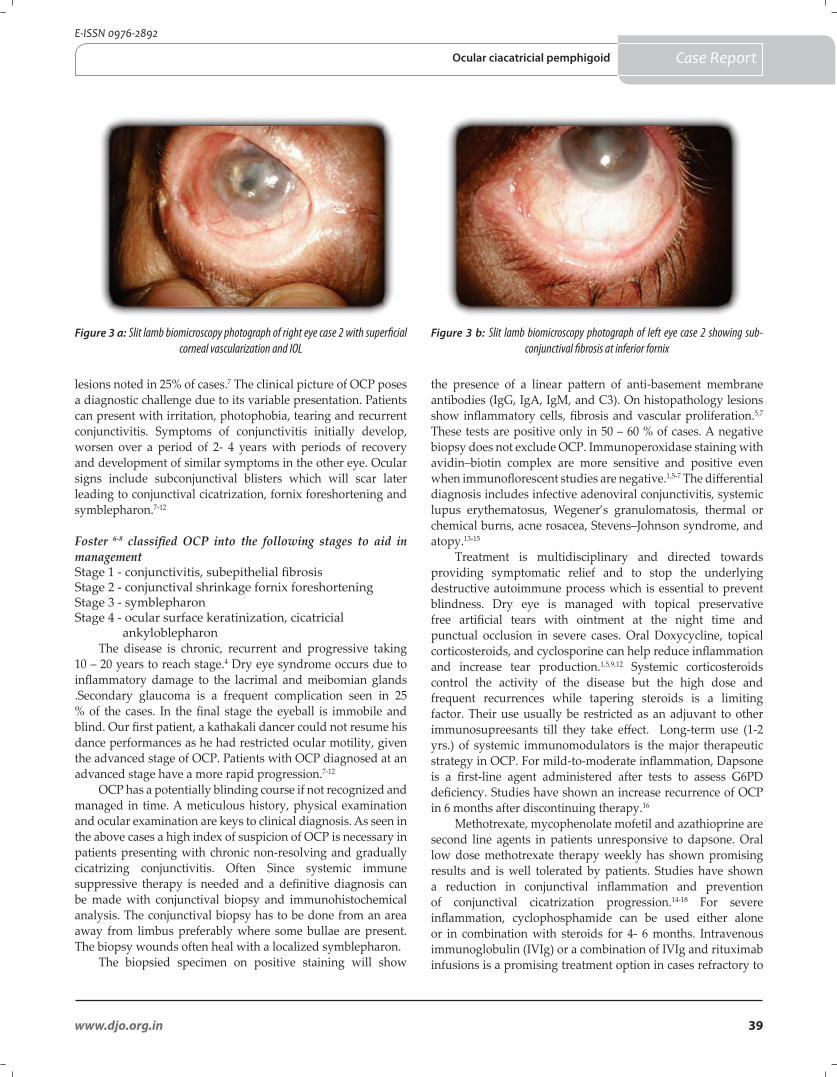
39www.djo.org.in
E-ISSN 0976-2892
lesions noted in 25% of cases.7 The clinical picture of OCP poses a diagnostic challenge due to its variable presentation. Patients can present with irritation, photophobia, tearing and recurrent conjunctivitis. Symptoms of conjunctivitis initially develop, worsen over a period of 2- 4 years with periods of recovery and development of similar symptoms in the other eye. Ocular signs include subconjunctival blisters which will scar later leading to conjunctival cicatrization, fornix foreshortening and symblepharon.7-12
Foster 6-8 classified OCP into the following stages to aid in management Stage 1 - conjunctivitis, subepithelial fibrosisStage 2 - conjunctival shrinkage fornix foreshorteningStage 3 - symblepharonStage 4 - ocular surface keratinization, cicatricial ankyloblepharon
The disease is chronic, recurrent and progressive taking 10 – 20 years to reach stage.4 Dry eye syndrome occurs due to inflammatory damage to the lacrimal and meibomian glands .Secondary glaucoma is a frequent complication seen in 25 % of the cases. In the final stage the eyeball is immobile and blind. Our first patient, a kathakali dancer could not resume his dance performances as he had restricted ocular motility, given the advanced stage of OCP. Patients with OCP diagnosed at an advanced stage have a more rapid progression.7-12
OCP has a potentially blinding course if not recognized and managed in time. A meticulous history, physical examination and ocular examination are keys to clinical diagnosis. As seen in the above cases a high index of suspicion of OCP is necessary in patients presenting with chronic non-resolving and gradually cicatrizing conjunctivitis. Often Since systemic immune suppressive therapy is needed and a definitive diagnosis can be made with conjunctival biopsy and immunohistochemical analysis. The conjunctival biopsy has to be done from an area away from limbus preferably where some bullae are present. The biopsy wounds often heal with a localized symblepharon.
The biopsied specimen on positive staining will show
Figure 3 b: Slit lamb biomicroscopy photograph of left eye case 2 showing sub-conjunctival fibrosis at inferior fornix
Figure 3 a: Slit lamb biomicroscopy photograph of right eye case 2 with superficial corneal vascularization and IOL
the presence of a linear pattern of anti-basement membrane antibodies (IgG, IgA, IgM, and C3). On histopathology lesions show inflammatory cells, fibrosis and vascular proliferation.5,7 These tests are positive only in 50 – 60 % of cases. A negative biopsy does not exclude OCP. Immunoperoxidase staining with avidin–biotin complex are more sensitive and positive even when immunoflorescent studies are negative.1,5-7 The differential diagnosis includes infective adenoviral conjunctivitis, systemic lupus erythematosus, Wegener’s granulomatosis, thermal or chemical burns, acne rosacea, Stevens–Johnson syndrome, and atopy.13-15
Treatment is multidisciplinary and directed towards providing symptomatic relief and to stop the underlying destructive autoimmune process which is essential to prevent blindness. Dry eye is managed with topical preservative free artificial tears with ointment at the night time and punctual occlusion in severe cases. Oral Doxycycline, topical corticosteroids, and cyclosporine can help reduce inflammation and increase tear production.1,5,9,12 Systemic corticosteroids control the activity of the disease but the high dose and frequent recurrences while tapering steroids is a limiting factor. Their use usually be restricted as an adjuvant to other immunosupreesants till they take effect. Long-term use (1-2 yrs.) of systemic immunomodulators is the major therapeutic strategy in OCP. For mild-to-moderate inflammation, Dapsone is a first-line agent administered after tests to assess G6PD deficiency. Studies have shown an increase recurrence of OCP in 6 months after discontinuing therapy.16
Methotrexate, mycophenolate mofetil and azathioprine are second line agents in patients unresponsive to dapsone. Oral low dose methotrexate therapy weekly has shown promising results and is well tolerated by patients. Studies have shown a reduction in conjunctival inflammation and prevention of conjunctival cicatrization progression.14-18 For severe inflammation, cyclophosphamide can be used either alone or in combination with steroids for 4- 6 months. Intravenous immunoglobulin (IVIg) or a combination of IVIg and rituximab infusions is a promising treatment option in cases refractory to
Case ReportOcular ciacatricial pemphigoid

40 Del J Ophthalmol 2013;24(1)
ISSN 0972-0200
other forms of immunosuppression but high cost is a limiting factor.17-18
Surgical intervention for co-morbid conditions like cataract or glaucoma or as rehabilitation to reconstruct the ocular surface should be attempted only after controlling the disease with adequate immunosuppressive therapy. As in our second patient, prior right eye surgery unmasked the disease while a successful cataract surgery was performed later once the disease was controlled with immunosuppressive agents. Corneal transplant has a poor prognosis due to presence of a dry eye, limbal stem cell deficiency and impaired lid function. In advance OCP, keratoprosthesis can be done for visual rehabilitation.
Conclusion
Early diagnosis and treatment are essential to achieving permanent remission. Delay in diagnosis and therapy leads to progression and eventually blindness. Current research has identified on the gene that predisposes to OCP and the target antigen. This will help develop newer diagnostic and therapeutic strategies to manage OCP.
References
1. Foster CS. Cicatricial pemphigoid. In: Krachmer JH, Mannis MJ, Holland EJ, editors. Cornea.Volume One: Fundamentals, Diagnosis and Management, 3rd ed. Philadelphia, PA: Mosby Elsevier; 2011:591–599.
2. Razzaque MS, Foster CS, Ahmed AR. Tissue and molecular events in human conjunctival scarring in ocular cicatricial pemphigoid. Histopathol 2001; 16:1203-12.
3. Tyagi S, Bhol K, Natarajan K, Livir-Rallatos C, Foster CS, Ahmed AR. Ocular cicatricial pemphigoid antigens: partial sequence and characterization. Proc Natl Acad Sci USA 1996; 93:14714–9.
4. Ahmed M, Zein G, Khawaja F, Foster CS. Ocular cicatricial pemphigoid: pathogenesis, diagnosis and treatment. Prog Retin Eye Res 2004; 23:579–92.
5. Brydak-Godowska J, Moneta-Wielgos J, Pauk-Domanska M, Drobecka-Brydak E, Samsel A,Kecik M, Kowalewski C et al. Diagnostics and pharmacological treatment of OCP cicatrical Pemphigoid. Klin Oczna 2005; 107:725.
6. Muna A, Foster CS. Ocular Cicatricial Pemphigoid in Uveitis and immunological disorders. Editors: Pleyer, U., Mondino, B., Berlin: Springer-Verlag; 2005.
7. Braun-Falco O, Plewig G, Wolff HH, Burgdorf WHC, eds. Dermatology. 2nd completely revised edition. Berlin: Springer-Verlag, 2000.
8. Foster CS, Wilson LA, Ekins MB. Immunosuppressive therapy for progressive ocular cicatricial pemphigoid. Ophthalmology 1982; 89:340–53.
9. Foster CS. Cicatricial Pemphigoid: eMedicine Ophthalmology. 2008 Dec; [cited 2010 Aug 7]
10. Kurihara M, Nishimur F, Hashimoto T, Komai A, Ueda H, Kokeguchi S et al. Pemphigus conjunctivae with scarring of the skin. Arch Dermatol Syph 1942; 46: 875-80.
11. Messmer EM, Hintschich CR, Partscht K, Messer G, Kampik A. OCP cicatricial pemphigoid. Retrospective analysis of risk factors and complications. Ophthalmology 2000; 97:113-20.
12. Hammer LH, Perry HD, Donnenfeld ED, Rahn EK. Symblepharon formation in epidemic keratoconjunctivitis.Cornea 1990; 9:338–40.
13. Jordan DR, Zafar A, Brownstein S, Faraji H. Cicatricial conjunctival inflammation with trichiasis as the presenting feature of Wegener granulomatosis. Ophthal Plast Reconstr Surg 2006; 22:69–71.
14. Chang JH, McCluskey PJ. OCP Cicatricial pemphigoid: manifestations and management. Curr Allergy Asthma Rep 2005; 5:333-8.
15. Kirzhner M, Jakobiec FA. Ocular cicatricial pemphigoid: a review of clinical features, immunopathology, differential diagnosis, and current management. Semin Ophthalmol 2011; 26:270–7.
16. Wozel G, Barth J. Current aspects of modes of action of dapsone. Int J Dermatol 1988; 27:547–52.
17. Saw VP, Dart JK, Rauz S, et al. Immunosuppressive therapy for ocular mucous membrane pemphigoid strategies and outcomes. Ophthalmology 2008; 115:253–61.
18. Durrani K, Zakka FR, Ahmed M, Memon M, Siddique SS, Foster CS. Systemic therapy with conventional and novel immunomodulatory agents for ocular inflammatory disease. Surv Ophthalmol 2011; 56: 474–510.
Case Report Revathi R et al
41www.djo.org.in
E-ISSN 0976-2892
No-Assistant Technique: Simplified Haptic Externalization For Glued IOL Delhi J Ophthalmol 2013; 24 (1): 41-42
A modified technique for externalizing the haptics in the Agarwal method of glued intrascleral fixation of a posterior chamber intraocular lens (IOL) is described. This technique eliminates the role of an assistant in holding the haptic during the entire surgical manoeuvre and subsequent complications associated with inappropriate handling of the haptic. The technique was used in 45 cases and was reproducible in all cases with no intraoperative complications. This technique is an attempt to make the process of haptic externalization, considered the most technically demanding part of the surgery, more easy and feasible.
*Priya NarangNarang Eye Care & Laser Centre,Ahmedabad, India.
*Author for correspondence
Tecnique DescriptionFibrin glue–assisted intrascleral haptic
fixation, as described by Agarwal et al1, is a well-established method of intraocular lens (IOL) fixation in cases of posterior capsule dehiscence. It requires an assistant to hold the leading haptic until the trailing haptic has been externalized and both haptics are free from their respective sclerotomy sites. Inappropriate handling of the leading haptic can lead to complications such as IOL torsion; haptic disfigurement; i.e.kinking or breaking of the haptic that requires IOL exchange; haptic slippage into the eye; or a dropped
IOL. Various methods to prevent the leading haptic from slipping back into the eye have been described. The sponge tire of an iris or capsule retractor (described by Dr.George Beiko and Dr.Roger Steinert2) is used to plug onto the haptic so that an assistant is not required to hold the haptic.
I describe a modified technique for externalizing the haptic that eliminates the role of an assistant in holding the leading haptic and prevents slippage of the leading haptic into the eye during externalization of the trailing haptic.3 This method makes the surgery more surgeon dependent than assistant dependent and prevents the complications that can occur because of inappropriate handling of the leading haptic. It allows the surgeon to safely and effectively externalize the haptics.
PrincipleThe modified haptic externalization
technique works on the principle of vector forces. The mid-pupillary plane is a major contributor to the success of the technique. The direction of vector forces change completely once the trailing haptic reaches or crosses the mid-pupillary plane. This causes further extrusion of the leading haptic from the sclerotomy site and eliminates the need for an assistant.
Surgical TechniqueTwo partial thickness scleral flaps of
2.5 by 2.5 mm are fashioned approximately 180 degree opposite to each other. An anterior chamber maintainer is introduced into the eye from a side port incision. Sclerotomy wound is created with a 20 G needle beneath both the scleral flaps approximately 1.5 mm from the limbus. The needle is directed obliquely downwards towards the mid vitreous cavity. A 23 G vitrectomy cutter is introduced from the sclerotomy site and thorough vitrectomy is done.
A 2.8 mm corneal tunnel is fashioned and an additional side port incision is created between the left sclerotomy site and the corneal tunnel. A 3 piece foldable IOL is loaded into the cartridge and the tip of the haptic is slightly protruded from the cartridge. The cartridge is introduced into the eye and the tip of the haptic is caught by the glued IOL forceps introduced from
Keywords : glued IOL forceps • fibrin glue • no-assistant
Priya Narang MS
Narang Eye Care & Laser Centre,Ahmedabad, iIndia - 380009email: [email protected]
Techniques
View Video on DJO Web Page: www.djo.org.in
DOI: http://dx.doi.org/10.7869/djo.2013.8

42 Del J Ophthalmol 2013;24(1)
ISSN 0972-0200
the left sclerotomy site. The IOL is slowly injected and the cartridge is slightly withdrawn so that the trailing haptic lies at the corneal incision. Once the entire IOL has unfolded, the leading haptic is pulled and externalized.
The trailing haptic is grasped and flexed into the eye with the glued IOL forceps towards 6’o clock position. This causes more extrusion of the leading haptic from the left sclerotomy site. A second glued IOL forceps is introduced from the side port incision and the tip of the trailing haptic is transferred to the left hand. The right handed glued IOL forceps is withdrawn from the eye and is reintroduced from the right sclerotomy site. The tip of the trailing haptic is now transferred from the left to the right hand (Handshake technique). The trailing haptic is then pulled and externalized from the right sclerotomy site.
Scleral pockets are created with a 26 G needle parallel to the sclerotomy site along the edge of the flap. The haptics are then tucked into these pockets and vitrectomy is done at the sclerotomy site to cut out any vitreous strands protruding from the site. The infusion is stopped; air bubble is injected and the bed of the scleral flap is dried with cotton swab. Fibrin glue is applied at the base of these flaps and is pressed for nearly 15 seconds. The remaining glue can be used to seal all the corneal incisions and the conjunctiva.
Financial & competing interest disclosureThe author does not have any competing interests in any product / proce-dure mentioned in this study. The author has no financial interests in any product / procedure mentioned in this study
References
1. 1. Agarwal A, Kumar DA, Jacob S, Baid C, Agarwal A, Srinivasan S. Fibrin glue–assisted sutureless posterior chamber intraocular lens implantation in eyes with deficient posterior capsules. J Cataract Refract Surg. 2008; 34:1433–8.
2. Beiko G, Steinert R: Modification of externalized haptic support of glued intraocular lens technique. J Cataract Refract Surg. 2013; 39:323-5.
3. Narang P. Modified method of haptic externalization of posterior chamber intraocular lens in fibrin glue assisted intrascleral fixation: No-assistant technique. J Cataract Refract Surg. 2013; 39:4-7.
Techniques Narang P
View Video on DJO Web Page: www.djo.org.in
Presented in part in the
ASCRS Symposium, San Francisco, CA , 2013
We welcome all DOS Members to actively contribute good quality manuscripts for the various section of of Delhi Journal of Ophthalmology – ORIGINAL ARTICLES, MAJOR REVIEWS, RECENT ADVANCES, and ALLIED OPHTHALMIC SCIENCES.
Please ensure that your submissions conform to the requirements of journal in order ensure speedy processing of the review of the manuscript.
We, at the editorial office of Delhi Journal of Ophthalmology, welcome your comments and suggestions on the new outlook of the Delhi Journal of Ophthalmology
Dr M.VANATHI MDEditor-in-chief
Delhi Journal of Ophthalmology
Announcement
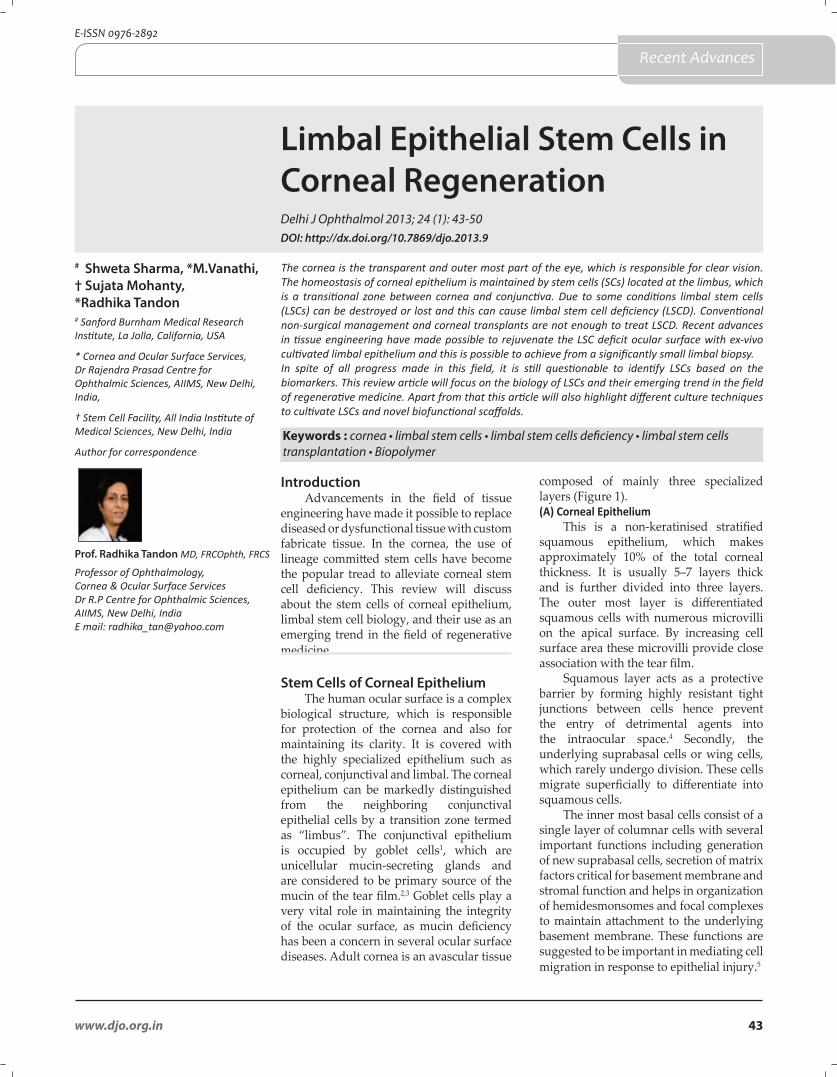
43www.djo.org.in
E-ISSN 0976-2892
Limbal Epithelial Stem Cells in Corneal Regeneration Delhi J Ophthalmol 2013; 24 (1): 43-50
The cornea is the transparent and outer most part of the eye, which is responsible for clear vision. The homeostasis of corneal epithelium is maintained by stem cells (SCs) located at the limbus, which is a transitional zone between cornea and conjunctiva. Due to some conditions limbal stem cells (LSCs) can be destroyed or lost and this can cause limbal stem cell deficiency (LSCD). Conventional non-surgical management and corneal transplants are not enough to treat LSCD. Recent advances in tissue engineering have made possible to rejuvenate the LSC deficit ocular surface with ex-vivo cultivated limbal epithelium and this is possible to achieve from a significantly small limbal biopsy.In spite of all progress made in this field, it is still questionable to identify LSCs based on the biomarkers. This review article will focus on the biology of LSCs and their emerging trend in the field of regenerative medicine. Apart from that this article will also highlight different culture techniques to cultivate LSCs and novel biofunctional scaffolds.
# Shweta Sharma, *M.Vanathi, † Sujata Mohanty, *Radhika Tandon# Sanford Burnham Medical Research Institute, La Jolla, California, USA
* Cornea and Ocular Surface Services, Dr Rajendra Prasad Centre for Ophthalmic Sciences, AIIMS, New Delhi, India,
† Stem Cell Facility, All India Institute of Medical Sciences, New Delhi, India
Author for correspondence
IntroductionAdvancements in the field of tissue
engineering have made it possible to replace diseased or dysfunctional tissue with custom fabricate tissue. In the cornea, the use of lineage committed stem cells have become the popular tread to alleviate corneal stem cell deficiency. This review will discuss about the stem cells of corneal epithelium, limbal stem cell biology, and their use as an emerging trend in the field of regenerative medicine.
Stem Cells of Corneal EpitheliumThe human ocular surface is a complex
biological structure, which is responsible for protection of the cornea and also for maintaining its clarity. It is covered with the highly specialized epithelium such as corneal, conjunctival and limbal. The corneal epithelium can be markedly distinguished from the neighboring conjunctival epithelial cells by a transition zone termed as “limbus”. The conjunctival epithelium is occupied by goblet cells1, which are unicellular mucin-secreting glands and are considered to be primary source of the mucin of the tear film.2,3 Goblet cells play a very vital role in maintaining the integrity of the ocular surface, as mucin deficiency has been a concern in several ocular surface diseases. Adult cornea is an avascular tissue
composed of mainly three specialized layers (Figure 1).(A) Corneal Epithelium
This is a non-keratinised stratified squamous epithelium, which makes approximately 10% of the total corneal thickness. It is usually 5–7 layers thick and is further divided into three layers. The outer most layer is differentiated squamous cells with numerous microvilli on the apical surface. By increasing cell surface area these microvilli provide close association with the tear film.
Squamous layer acts as a protective barrier by forming highly resistant tight junctions between cells hence prevent the entry of detrimental agents into the intraocular space.4 Secondly, the underlying suprabasal cells or wing cells, which rarely undergo division. These cells migrate superficially to differentiate into squamous cells.
The inner most basal cells consist of a single layer of columnar cells with several important functions including generation of new suprabasal cells, secretion of matrix factors critical for basement membrane and stromal function and helps in organization of hemidesmonsomes and focal complexes to maintain attachment to the underlying basement membrane. These functions are suggested to be important in mediating cell migration in response to epithelial injury.5
Keywords : cornea • limbal stem cells • limbal stem cells deficiency • limbal stem cells transplantation • Biopolymer
Prof. Radhika Tandon MD, FRCOphth, FRCS
Professor of Ophthalmology, Cornea & Ocular Surface ServicesDr R.P Centre for Ophthalmic Sciences, AIIMS, New Delhi, IndiaE mail: [email protected]
Recent Advances
DOI: http://dx.doi.org/10.7869/djo.2013.9
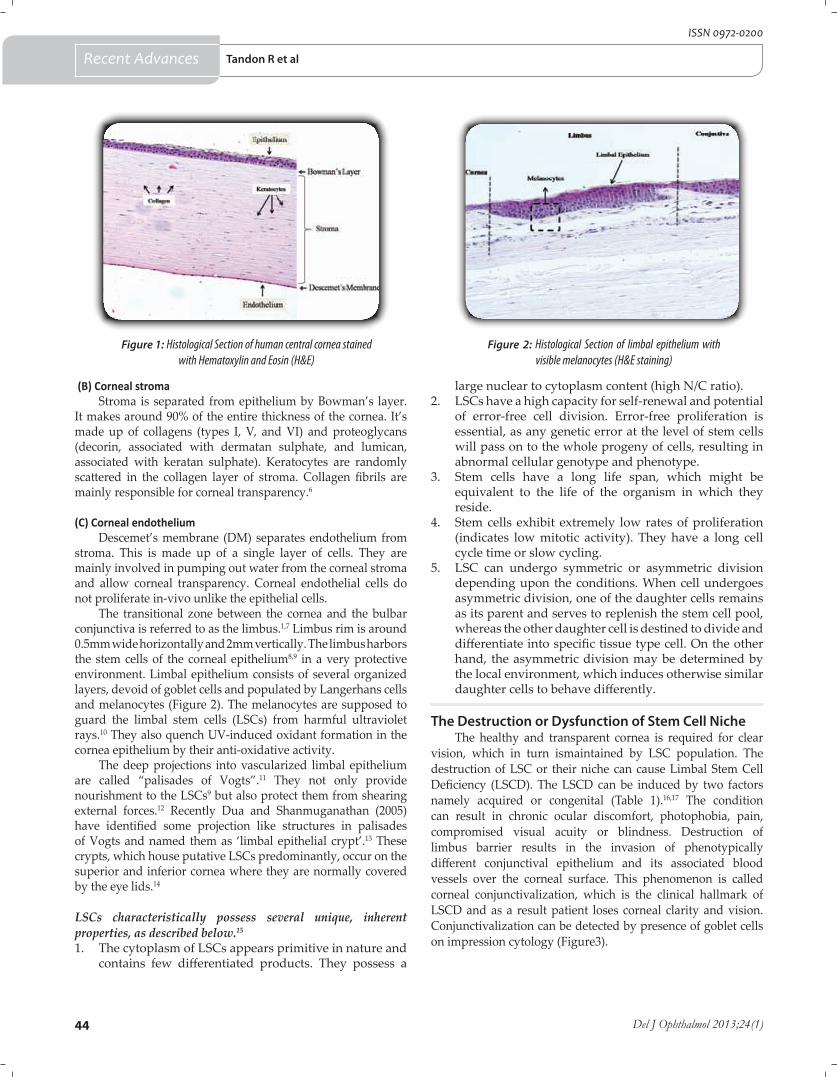
44 Del J Ophthalmol 2013;24(1)
ISSN 0972-0200
(B) Corneal stromaStroma is separated from epithelium by Bowman’s layer.
It makes around 90% of the entire thickness of the cornea. It’s made up of collagens (types I, V, and VI) and proteoglycans (decorin, associated with dermatan sulphate, and lumican, associated with keratan sulphate). Keratocytes are randomly scattered in the collagen layer of stroma. Collagen fibrils are mainly responsible for corneal transparency.6
(C) Corneal endothelium
Descemet’s membrane (DM) separates endothelium from stroma. This is made up of a single layer of cells. They are mainly involved in pumping out water from the corneal stroma and allow corneal transparency. Corneal endothelial cells do not proliferate in-vivo unlike the epithelial cells.
The transitional zone between the cornea and the bulbar conjunctiva is referred to as the limbus.1,7 Limbus rim is around 0.5mm wide horizontally and 2mm vertically. The limbus harbors the stem cells of the corneal epithelium8,9 in a very protective environment. Limbal epithelium consists of several organized layers, devoid of goblet cells and populated by Langerhans cells and melanocytes (Figure 2). The melanocytes are supposed to guard the limbal stem cells (LSCs) from harmful ultraviolet rays.10 They also quench UV-induced oxidant formation in the cornea epithelium by their anti-oxidative activity.
The deep projections into vascularized limbal epithelium are called “palisades of Vogts”.11 They not only provide nourishment to the LSCs9 but also protect them from shearing external forces.12 Recently Dua and Shanmuganathan (2005) have identified some projection like structures in palisades of Vogts and named them as ‘limbal epithelial crypt’.13 These crypts, which house putative LSCs predominantly, occur on the superior and inferior cornea where they are normally covered by the eye lids.14
LSCs characteristically possess several unique, inherent properties, as described below.15
1. The cytoplasm of LSCs appears primitive in nature and contains few differentiated products. They possess a
large nuclear to cytoplasm content (high N/C ratio). 2. LSCs have a high capacity for self-renewal and potential
of error-free cell division. Error-free proliferation is essential, as any genetic error at the level of stem cells will pass on to the whole progeny of cells, resulting in abnormal cellular genotype and phenotype.
3. Stem cells have a long life span, which might be equivalent to the life of the organism in which they reside.
4. Stem cells exhibit extremely low rates of proliferation (indicates low mitotic activity). They have a long cell cycle time or slow cycling.
5. LSC can undergo symmetric or asymmetric division depending upon the conditions. When cell undergoes asymmetric division, one of the daughter cells remains as its parent and serves to replenish the stem cell pool, whereas the other daughter cell is destined to divide and differentiate into specific tissue type cell. On the other hand, the asymmetric division may be determined by the local environment, which induces otherwise similar daughter cells to behave differently.
The Destruction or Dysfunction of Stem Cell NicheThe healthy and transparent cornea is required for clear
vision, which in turn ismaintained by LSC population. The destruction of LSC or their niche can cause Limbal Stem Cell Deficiency (LSCD). The LSCD can be induced by two factors namely acquired or congenital (Table 1).16,17 The condition can result in chronic ocular discomfort, photophobia, pain, compromised visual acuity or blindness. Destruction of limbus barrier results in the invasion of phenotypically different conjunctival epithelium and its associated blood vessels over the corneal surface. This phenomenon is called corneal conjunctivalization, which is the clinical hallmark of LSCD and as a result patient loses corneal clarity and vision. Conjunctivalization can be detected by presence of goblet cells on impression cytology (Figure3).
Figure 1: Histological Section of human central cornea stained with Hematoxylin and Eosin (H&E)
Figure 2: Histological Section of limbal epithelium with visible melanocytes (H&E staining)
Tandon R et alRecent Advances
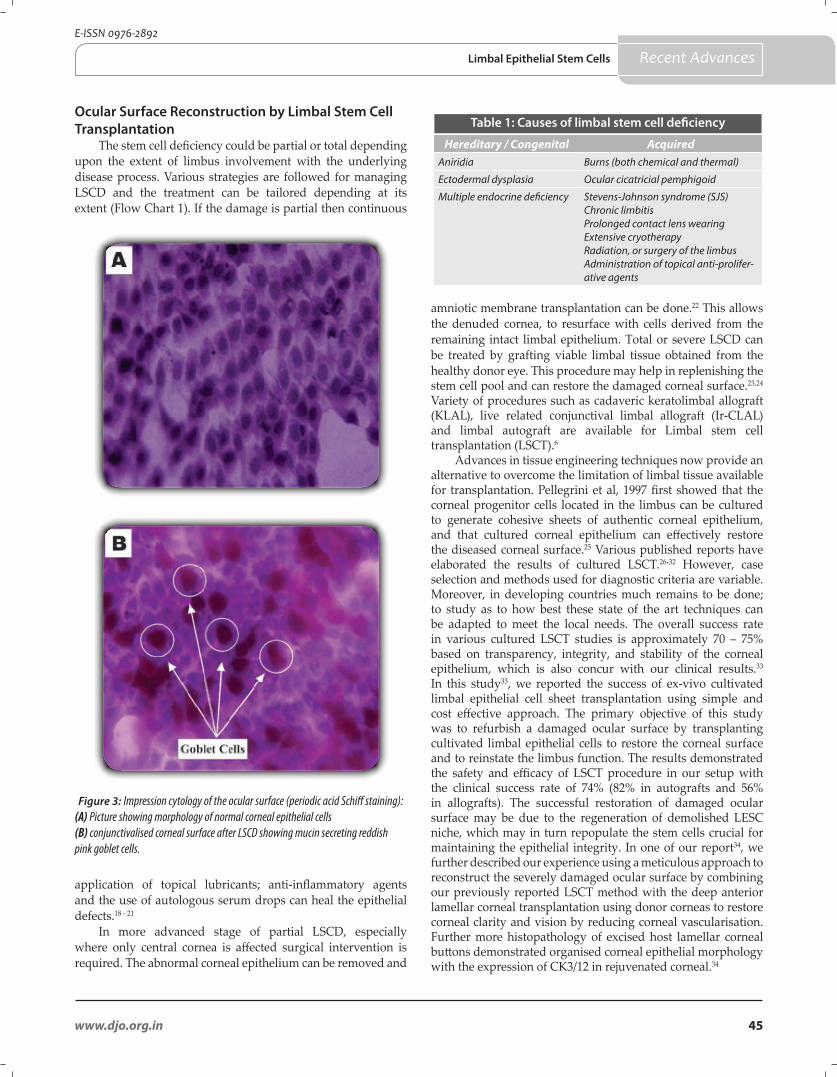
45www.djo.org.in
E-ISSN 0976-2892
Figure 3: Impression cytology of the ocular surface (periodic acid Schiff staining): (A) Picture showing morphology of normal corneal epithelial cells (B) conjunctivalised corneal surface after LSCD showing mucin secreting reddish pink goblet cells.
Ocular Surface Reconstruction by Limbal Stem Cell Transplantation
The stem cell deficiency could be partial or total depending upon the extent of limbus involvement with the underlying disease process. Various strategies are followed for managing LSCD and the treatment can be tailored depending at its extent (Flow Chart 1). If the damage is partial then continuous
application of topical lubricants; anti-inflammatory agents and the use of autologous serum drops can heal the epithelial defects.18 - 21
In more advanced stage of partial LSCD, especially where only central cornea is affected surgical intervention is required. The abnormal corneal epithelium can be removed and
Limbal Epithelial Stem Cells
amniotic membrane transplantation can be done.22 This allows the denuded cornea, to resurface with cells derived from the remaining intact limbal epithelium. Total or severe LSCD can be treated by grafting viable limbal tissue obtained from the healthy donor eye. This procedure may help in replenishing the stem cell pool and can restore the damaged corneal surface.23,24 Variety of procedures such as cadaveric keratolimbal allograft (KLAL), live related conjunctival limbal allograft (Ir-CLAL) and limbal autograft are available for Limbal stem cell transplantation (LSCT).6
Advances in tissue engineering techniques now provide an alternative to overcome the limitation of limbal tissue available for transplantation. Pellegrini et al, 1997 first showed that the corneal progenitor cells located in the limbus can be cultured to generate cohesive sheets of authentic corneal epithelium, and that cultured corneal epithelium can effectively restore the diseased corneal surface.25 Various published reports have elaborated the results of cultured LSCT.26-32 However, case selection and methods used for diagnostic criteria are variable. Moreover, in developing countries much remains to be done; to study as to how best these state of the art techniques can be adapted to meet the local needs. The overall success rate in various cultured LSCT studies is approximately 70 – 75% based on transparency, integrity, and stability of the corneal epithelium, which is also concur with our clinical results.33 In this study33, we reported the success of ex-vivo cultivated limbal epithelial cell sheet transplantation using simple and cost effective approach. The primary objective of this study was to refurbish a damaged ocular surface by transplanting cultivated limbal epithelial cells to restore the corneal surface and to reinstate the limbus function. The results demonstrated the safety and efficacy of LSCT procedure in our setup with the clinical success rate of 74% (82% in autografts and 56% in allografts). The successful restoration of damaged ocular surface may be due to the regeneration of demolished LESC niche, which may in turn repopulate the stem cells crucial for maintaining the epithelial integrity. In one of our report34, we further described our experience using a meticulous approach to reconstruct the severely damaged ocular surface by combining our previously reported LSCT method with the deep anterior lamellar corneal transplantation using donor corneas to restore corneal clarity and vision by reducing corneal vascularisation. Further more histopathology of excised host lamellar corneal buttons demonstrated organised corneal epithelial morphology with the expression of CK3/12 in rejuvenated corneal.34
Hereditary / Congenital AcquiredAniridia Burns (both chemical and thermal)
Ectodermal dysplasia Ocular cicatricial pemphigoid
Multiple endocrine deficiency Stevens-Johnson syndrome (SJS)Chronic limbitisProlonged contact lens wearingExtensive cryotherapyRadiation, or surgery of the limbusAdministration of topical anti-prolifer-ative agents
Table 1: Causes of limbal stem cell deficiency
Recent Advances
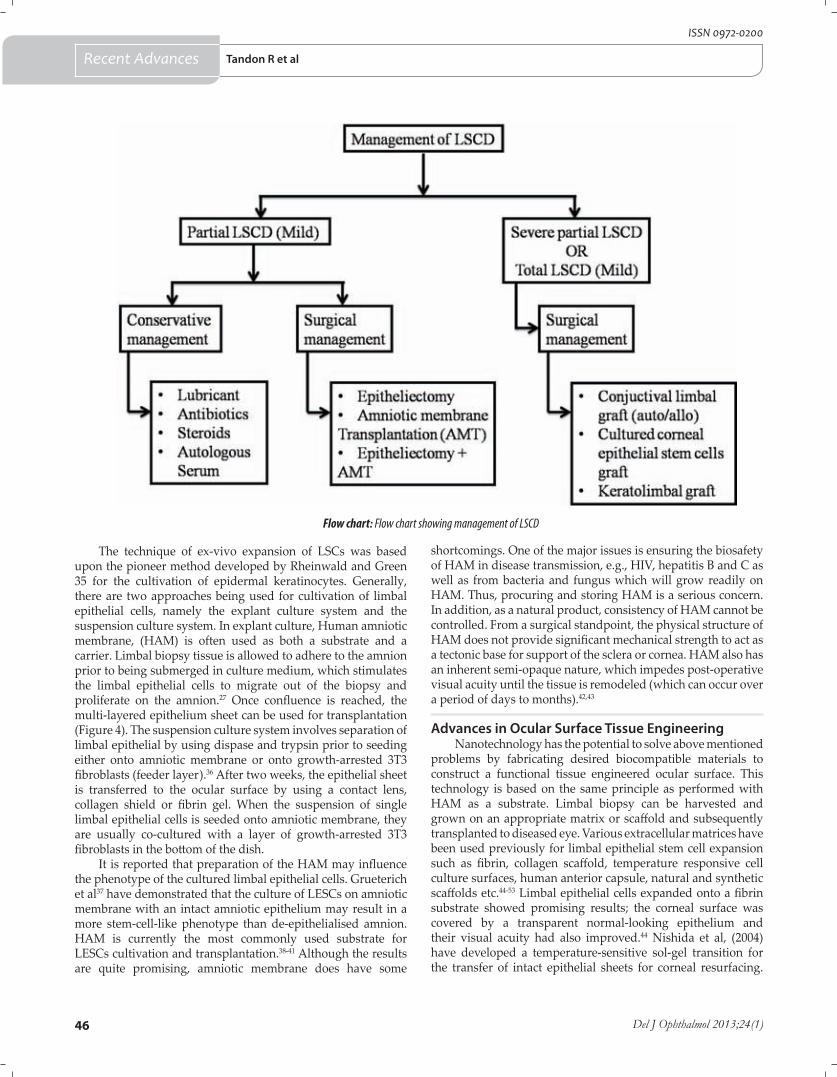
46 Del J Ophthalmol 2013;24(1)
ISSN 0972-0200
The technique of ex-vivo expansion of LSCs was based upon the pioneer method developed by Rheinwald and Green 35 for the cultivation of epidermal keratinocytes. Generally, there are two approaches being used for cultivation of limbal epithelial cells, namely the explant culture system and the suspension culture system. In explant culture, Human amniotic membrane, (HAM) is often used as both a substrate and a carrier. Limbal biopsy tissue is allowed to adhere to the amnion prior to being submerged in culture medium, which stimulates the limbal epithelial cells to migrate out of the biopsy and proliferate on the amnion.27 Once confluence is reached, the multi-layered epithelium sheet can be used for transplantation (Figure 4). The suspension culture system involves separation of limbal epithelial by using dispase and trypsin prior to seeding either onto amniotic membrane or onto growth-arrested 3T3 fibroblasts (feeder layer).36 After two weeks, the epithelial sheet is transferred to the ocular surface by using a contact lens, collagen shield or fibrin gel. When the suspension of single limbal epithelial cells is seeded onto amniotic membrane, they are usually co-cultured with a layer of growth-arrested 3T3 fibroblasts in the bottom of the dish.
It is reported that preparation of the HAM may influence the phenotype of the cultured limbal epithelial cells. Grueterich et al37 have demonstrated that the culture of LESCs on amniotic membrane with an intact amniotic epithelium may result in a more stem-cell-like phenotype than de-epithelialised amnion. HAM is currently the most commonly used substrate for LESCs cultivation and transplantation.38-41 Although the results are quite promising, amniotic membrane does have some
shortcomings. One of the major issues is ensuring the biosafety of HAM in disease transmission, e.g., HIV, hepatitis B and C as well as from bacteria and fungus which will grow readily on HAM. Thus, procuring and storing HAM is a serious concern. In addition, as a natural product, consistency of HAM cannot be controlled. From a surgical standpoint, the physical structure of HAM does not provide significant mechanical strength to act as a tectonic base for support of the sclera or cornea. HAM also has an inherent semi-opaque nature, which impedes post-operative visual acuity until the tissue is remodeled (which can occur over a period of days to months).42,43
Advances in Ocular Surface Tissue EngineeringNanotechnology has the potential to solve above mentioned
problems by fabricating desired biocompatible materials to construct a functional tissue engineered ocular surface. This technology is based on the same principle as performed with HAM as a substrate. Limbal biopsy can be harvested and grown on an appropriate matrix or scaffold and subsequently transplanted to diseased eye. Various extracellular matrices have been used previously for limbal epithelial stem cell expansion such as fibrin, collagen scaffold, temperature responsive cell culture surfaces, human anterior capsule, natural and synthetic scaffolds etc.44-53 Limbal epithelial cells expanded onto a fibrin substrate showed promising results; the corneal surface was covered by a transparent normal-looking epithelium and their visual acuity had also improved.44 Nishida et al, (2004) have developed a temperature-sensitive sol-gel transition for the transfer of intact epithelial sheets for corneal resurfacing.
Flow chart: Flow chart showing management of LSCD
Recent Advances Tandon R et al
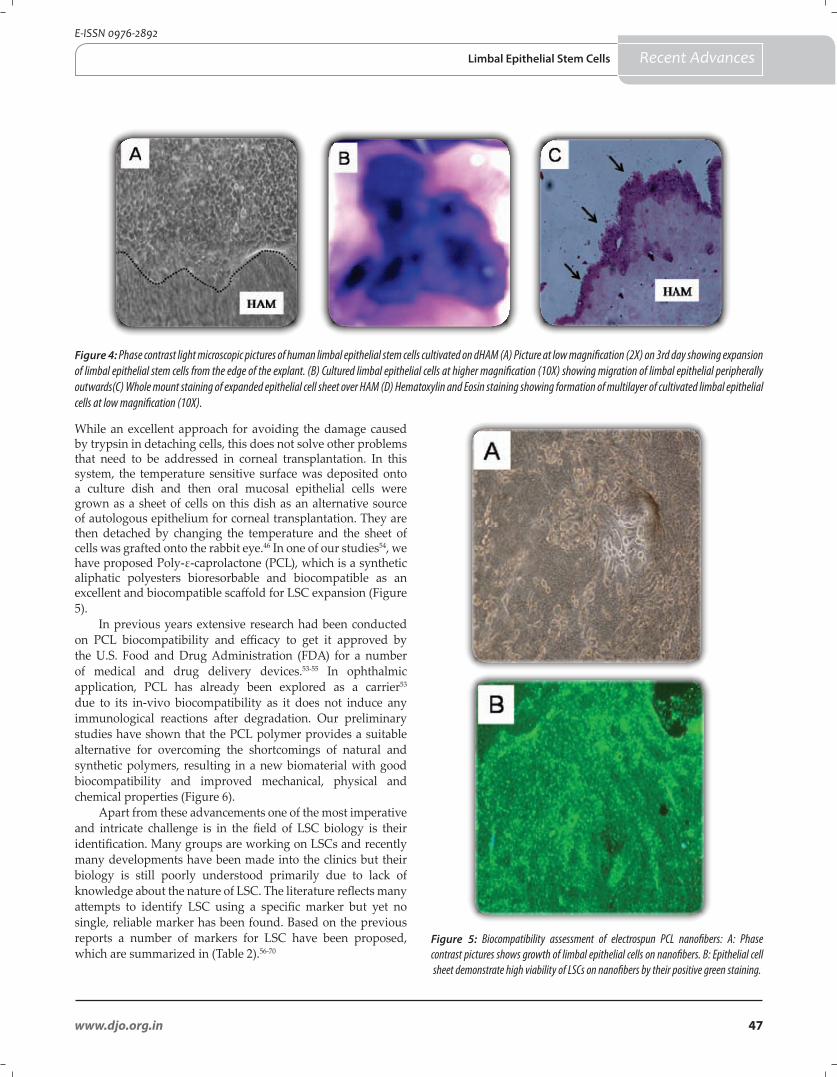
47www.djo.org.in
E-ISSN 0976-2892
While an excellent approach for avoiding the damage caused by trypsin in detaching cells, this does not solve other problems that need to be addressed in corneal transplantation. In this system, the temperature sensitive surface was deposited onto a culture dish and then oral mucosal epithelial cells were grown as a sheet of cells on this dish as an alternative source of autologous epithelium for corneal transplantation. They are then detached by changing the temperature and the sheet of cells was grafted onto the rabbit eye.46 In one of our studies54, we have proposed Poly-ε-caprolactone (PCL), which is a synthetic aliphatic polyesters bioresorbable and biocompatible as an excellent and biocompatible scaffold for LSC expansion (Figure 5).
In previous years extensive research had been conducted on PCL biocompatibility and efficacy to get it approved by the U.S. Food and Drug Administration (FDA) for a number of medical and drug delivery devices.53-55 In ophthalmic application, PCL has already been explored as a carrier53 due to its in-vivo biocompatibility as it does not induce any immunological reactions after degradation. Our preliminary studies have shown that the PCL polymer provides a suitable alternative for overcoming the shortcomings of natural and synthetic polymers, resulting in a new biomaterial with good biocompatibility and improved mechanical, physical and chemical properties (Figure 6).
Apart from these advancements one of the most imperative and intricate challenge is in the field of LSC biology is their identification. Many groups are working on LSCs and recently many developments have been made into the clinics but their biology is still poorly understood primarily due to lack of knowledge about the nature of LSC. The literature reflects many attempts to identify LSC using a specific marker but yet no single, reliable marker has been found. Based on the previous reports a number of markers for LSC have been proposed, which are summarized in (Table 2).56-70
Figure 4: Phase contrast light microscopic pictures of human limbal epithelial stem cells cultivated on dHAM (A) Picture at low magnification (2X) on 3rd day showing expansion of limbal epithelial stem cells from the edge of the explant. (B) Cultured limbal epithelial cells at higher magnification (10X) showing migration of limbal epithelial peripherally outwards(C) Whole mount staining of expanded epithelial cell sheet over HAM (D) Hematoxylin and Eosin staining showing formation of multilayer of cultivated limbal epithelial cells at low magnification (10X).
Figure 5: Biocompatibility assessment of electrospun PCL nanofibers: A: Phase contrast pictures shows growth of limbal epithelial cells on nanofibers. B: Epithelial cell sheet demonstrate high viability of LSCs on nanofibers by their positive green staining.
Recent AdvancesLimbal Epithelial Stem Cells
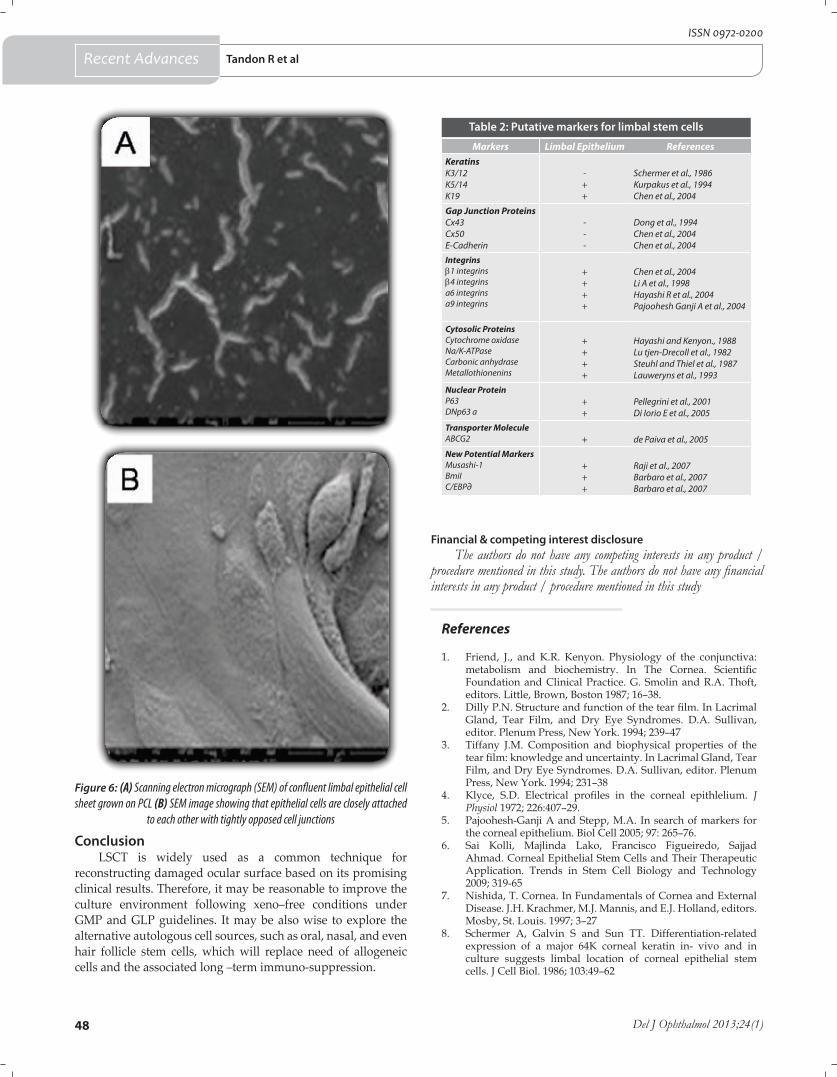
48 Del J Ophthalmol 2013;24(1)
ISSN 0972-0200
References
1. Friend, J., and K.R. Kenyon. Physiology of the conjunctiva: metabolism and biochemistry. In The Cornea. Scientific Foundation and Clinical Practice. G. Smolin and R.A. Thoft, editors. Little, Brown, Boston 1987; 16–38.
2. Dilly P.N. Structure and function of the tear film. In Lacrimal Gland, Tear Film, and Dry Eye Syndromes. D.A. Sullivan, editor. Plenum Press, New York. 1994; 239–47
3. Tiffany J.M. Composition and biophysical properties of the tear film: knowledge and uncertainty. In Lacrimal Gland, Tear Film, and Dry Eye Syndromes. D.A. Sullivan, editor. Plenum Press, New York. 1994; 231–38
4. Klyce, S.D. Electrical profiles in the corneal epithlelium. J Physiol 1972; 226:407–29.
5. Pajoohesh-Ganji A and Stepp, M.A. In search of markers for the corneal epithelium. Biol Cell 2005; 97: 265–76.
6. Sai Kolli, Majlinda Lako, Francisco Figueiredo, Sajjad Ahmad. Corneal Epithelial Stem Cells and Their Therapeutic Application. Trends in Stem Cell Biology and Technology 2009; 319-65
7. Nishida, T. Cornea. In Fundamentals of Cornea and External Disease. J.H. Krachmer, M.J. Mannis, and E.J. Holland, editors. Mosby, St. Louis. 1997; 3–27
8. Schermer A, Galvin S and Sun TT. Differentiation-related expression of a major 64K corneal keratin in- vivo and in culture suggests limbal location of corneal epithelial stem cells. J Cell Biol. 1986; 103:49–62
Figure 6: (A) Scanning electron micrograph (SEM) of confluent limbal epithelial cell sheet grown on PCL (B) SEM image showing that epithelial cells are closely attached
to each other with tightly opposed cell junctions
ConclusionLSCT is widely used as a common technique for
reconstructing damaged ocular surface based on its promising clinical results. Therefore, it may be reasonable to improve the culture environment following xeno–free conditions under GMP and GLP guidelines. It may be also wise to explore the alternative autologous cell sources, such as oral, nasal, and even hair follicle stem cells, which will replace need of allogeneic cells and the associated long –term immuno-suppression.
Markers Limbal Epithelium ReferencesKeratinsK3/12K5/14K19
-++
Schermer et al., 1986Kurpakus et al., 1994Chen et al., 2004
Gap Junction ProteinsCx43Cx50E-Cadherin
---
Dong et al., 1994Chen et al., 2004Chen et al., 2004
Integrinsb1 integrinsb4 integrinsa6 integrinsa9 integrins
++++
Chen et al., 2004Li A et al., 1998Hayashi R et al., 2004Pajoohesh Ganji A et al., 2004
Cytosolic ProteinsCytochrome oxidaseNa/K-ATPaseCarbonic anhydraseMetallothionenins
++++
Hayashi and Kenyon., 1988Lu tjen-Drecoll et al., 1982Steuhl and Thiel et al., 1987Lauweryns et al., 1993
Nuclear ProteinP63DNp63 a
++
Pellegrini et al., 2001Di Iorio E et al., 2005
Transporter MoleculeABCG2 + de Paiva et al., 2005
New Potential MarkersMusashi-1BmiIC/EBP∂
+++
Raji et al., 2007Barbaro et al., 2007Barbaro et al., 2007
Table 2: Putative markers for limbal stem cells
Financial & competing interest disclosureThe authors do not have any competing interests in any product /
procedure mentioned in this study. The authors do not have any financial interests in any product / procedure mentioned in this study
Recent Advances Tandon R et al
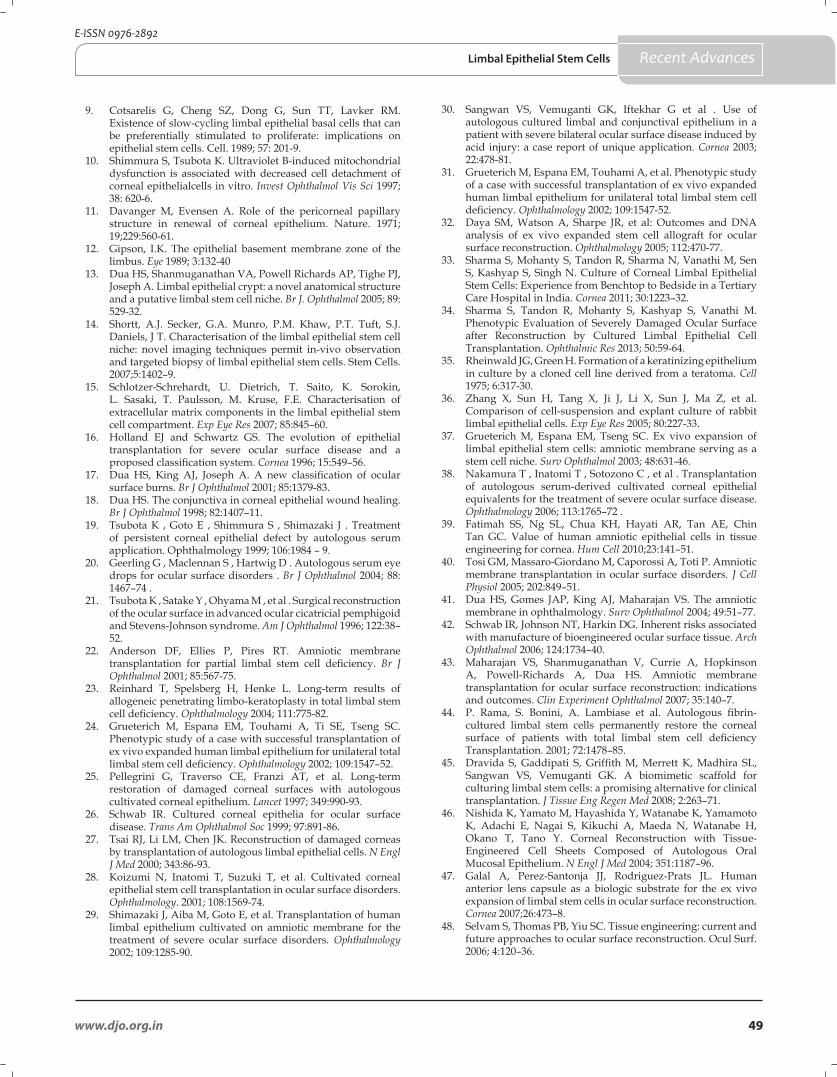
49www.djo.org.in
E-ISSN 0976-2892
9. Cotsarelis G, Cheng SZ, Dong G, Sun TT, Lavker RM. Existence of slow-cycling limbal epithelial basal cells that can be preferentially stimulated to proliferate: implications on epithelial stem cells. Cell. 1989; 57: 201-9.
10. Shimmura S, Tsubota K. Ultraviolet B-induced mitochondrial dysfunction is associated with decreased cell detachment of corneal epithelialcells in vitro. Invest Ophthalmol Vis Sci 1997; 38: 620-6.
11. Davanger M, Evensen A. Role of the pericorneal papillary structure in renewal of corneal epithelium. Nature. 1971; 19;229:560-61.
12. Gipson, I.K. The epithelial basement membrane zone of the limbus. Eye 1989; 3:132-40
13. Dua HS, Shanmuganathan VA, Powell Richards AP, Tighe PJ, Joseph A. Limbal epithelial crypt: a novel anatomical structure and a putative limbal stem cell niche. Br J. Ophthalmol 2005; 89: 529-32.
14. Shortt, A.J. Secker, G.A. Munro, P.M. Khaw, P.T. Tuft, S.J. Daniels, J T. Characterisation of the limbal epithelial stem cell niche: novel imaging techniques permit in-vivo observation and targeted biopsy of limbal epithelial stem cells. Stem Cells. 2007;5:1402–9.
15. Schlotzer-Schrehardt, U. Dietrich, T. Saito, K. Sorokin, L. Sasaki, T. Paulsson, M. Kruse, F.E. Characterisation of extracellular matrix components in the limbal epithelial stem cell compartment. Exp Eye Res 2007; 85:845–60.
16. Holland EJ and Schwartz GS. The evolution of epithelial transplantation for severe ocular surface disease and a proposed classification system. Cornea 1996; 15:549–56.
17. Dua HS, King AJ, Joseph A. A new classification of ocular surface burns. Br J Ophthalmol 2001; 85:1379-83.
18. Dua HS. The conjunctiva in corneal epithelial wound healing. Br J Ophthalmol 1998; 82:1407–11.
19. Tsubota K , Goto E , Shimmura S , Shimazaki J . Treatment of persistent corneal epithelial defect by autologous serum application. Ophthalmology 1999; 106:1984 – 9.
20. Geerling G , Maclennan S , Hartwig D . Autologous serum eye drops for ocular surface disorders . Br J Ophthalmol 2004; 88: 1467–74 .
21. Tsubota K , Satake Y , Ohyama M , et al . Surgical reconstruction of the ocular surface in advanced ocular cicatricial pemphigoid and Stevens-Johnson syndrome. Am J Ophthalmol 1996; 122:38–52.
22. Anderson DF, Ellies P, Pires RT. Amniotic membrane transplantation for partial limbal stem cell deficiency. Br J Ophthalmol 2001; 85:567-75.
23. Reinhard T, Spelsberg H, Henke L. Long-term results of allogeneic penetrating limbo-keratoplasty in total limbal stem cell deficiency. Ophthalmology 2004; 111:775-82.
24. Grueterich M, Espana EM, Touhami A, Ti SE, Tseng SC. Phenotypic study of a case with successful transplantation of ex vivo expanded human limbal epithelium for unilateral total limbal stem cell deficiency. Ophthalmology 2002; 109:1547–52.
25. Pellegrini G, Traverso CE, Franzi AT, et al. Long-term restoration of damaged corneal surfaces with autologous cultivated corneal epithelium. Lancet 1997; 349:990-93.
26. Schwab IR. Cultured corneal epithelia for ocular surface disease. Trans Am Ophthalmol Soc 1999; 97:891-86.
27. Tsai RJ, Li LM, Chen JK. Reconstruction of damaged corneas by transplantation of autologous limbal epithelial cells. N Engl J Med 2000; 343:86-93.
28. Koizumi N, Inatomi T, Suzuki T, et al. Cultivated corneal epithelial stem cell transplantation in ocular surface disorders. Ophthalmology. 2001; 108:1569-74.
29. Shimazaki J, Aiba M, Goto E, et al. Transplantation of human limbal epithelium cultivated on amniotic membrane for the treatment of severe ocular surface disorders. Ophthalmology 2002; 109:1285-90.
30. Sangwan VS, Vemuganti GK, Iftekhar G et al . Use of autologous cultured limbal and conjunctival epithelium in a patient with severe bilateral ocular surface disease induced by acid injury: a case report of unique application. Cornea 2003; 22:478-81.
31. Grueterich M, Espana EM, Touhami A, et al. Phenotypic study of a case with successful transplantation of ex vivo expanded human limbal epithelium for unilateral total limbal stem cell deficiency. Ophthalmology 2002; 109:1547-52.
32. Daya SM, Watson A, Sharpe JR, et al: Outcomes and DNA analysis of ex vivo expanded stem cell allograft for ocular surface reconstruction. Ophthalmology 2005; 112:470-77.
33. Sharma S, Mohanty S, Tandon R, Sharma N, Vanathi M, Sen S, Kashyap S, Singh N. Culture of Corneal Limbal Epithelial Stem Cells: Experience from Benchtop to Bedside in a Tertiary Care Hospital in India. Cornea 2011; 30:1223–32.
34. Sharma S, Tandon R, Mohanty S, Kashyap S, Vanathi M. Phenotypic Evaluation of Severely Damaged Ocular Surface after Reconstruction by Cultured Limbal Epithelial Cell Transplantation. Ophthalmic Res 2013; 50:59-64.
35. Rheinwald JG, Green H. Formation of a keratinizing epithelium in culture by a cloned cell line derived from a teratoma. Cell 1975; 6:317-30.
36. Zhang X, Sun H, Tang X, Ji J, Li X, Sun J, Ma Z, et al. Comparison of cell-suspension and explant culture of rabbit limbal epithelial cells. Exp Eye Res 2005; 80:227-33.
37. Grueterich M, Espana EM, Tseng SC. Ex vivo expansion of limbal epithelial stem cells: amniotic membrane serving as a stem cell niche. Surv Ophthalmol 2003; 48:631-46.
38. Nakamura T , Inatomi T , Sotozono C , et al . Transplantation of autologous serum-derived cultivated corneal epithelial equivalents for the treatment of severe ocular surface disease. Ophthalmology 2006; 113:1765–72 .
39. Fatimah SS, Ng SL, Chua KH, Hayati AR, Tan AE, Chin Tan GC. Value of human amniotic epithelial cells in tissue engineering for cornea. Hum Cell 2010;23:141–51.
40. Tosi GM, Massaro-Giordano M, Caporossi A, Toti P. Amniotic membrane transplantation in ocular surface disorders. J Cell Physiol 2005; 202:849–51.
41. Dua HS, Gomes JAP, King AJ, Maharajan VS. The amniotic membrane in ophthalmology. Surv Ophthalmol 2004; 49:51–77.
42. Schwab IR, Johnson NT, Harkin DG. Inherent risks associated with manufacture of bioengineered ocular surface tissue. Arch Ophthalmol 2006; 124:1734–40.
43. Maharajan VS, Shanmuganathan V, Currie A, Hopkinson A, Powell-Richards A, Dua HS. Amniotic membrane transplantation for ocular surface reconstruction: indications and outcomes. Clin Experiment Ophthalmol 2007; 35:140–7.
44. P. Rama, S. Bonini, A. Lambiase et al. Autologous fibrin-cultured limbal stem cells permanently restore the corneal surface of patients with total limbal stem cell deficiency Transplantation. 2001; 72:1478–85.
45. Dravida S, Gaddipati S, Griffith M, Merrett K, Madhira SL, Sangwan VS, Vemuganti GK. A biomimetic scaffold for culturing limbal stem cells: a promising alternative for clinical transplantation. J Tissue Eng Regen Med 2008; 2:263–71.
46. Nishida K, Yamato M, Hayashida Y, Watanabe K, Yamamoto K, Adachi E, Nagai S, Kikuchi A, Maeda N, Watanabe H, Okano T, Tano Y. Corneal Reconstruction with Tissue-Engineered Cell Sheets Composed of Autologous Oral Mucosal Epithelium. N Engl J Med 2004; 351:1187–96.
47. Galal A, Perez-Santonja JJ, Rodriguez-Prats JL. Human anterior lens capsule as a biologic substrate for the ex vivo expansion of limbal stem cells in ocular surface reconstruction. Cornea 2007;26:473–8.
48. Selvam S, Thomas PB, Yiu SC. Tissue engineering: current and future approaches to ocular surface reconstruction. Ocul Surf. 2006; 4:120–36.
Recent AdvancesLimbal Epithelial Stem Cells
50 Del J Ophthalmol 2013;24(1)
ISSN 0972-0200
49. Chen J, Li Q, Xu J, Huang Y, Ding Y, Deng H, Zhao S, Chen R. Study on biocompatibility of complexes of collagen-chitosan-sodium hyaluronate and cornea. Artif Organs 2005; 29:104–13.
50. 37. Yeh LK, Chen Y, Chiu C, Hu F, Young T, Wang I. The phenotype of bovine corneal epithelial cells on chitosan membrane. J Biomed Mater Res A 2009; 90:18–26.
51. Sudha B, Madhavan HN, Sitalakshmi G, Malathi J, Krishnakumar S, Mori Y, Yoshioka H, Abraham S. Cultivation of human corneal limbal stem cells in Mebiol gel® - A thermoreversible gelation polymer. Indian J Med Res 2006; 124:655–64.
52. Alaminos M, Del Carmen S’anchez-Quevedo M. Mu˜noz-Avila JI. Construction of a complete rabbit cornea substitute using a fibrin–agarose scaffold. Invest Ophthalmol Vis Sci 2006; 47:3311–7.
53. Ang LP, Cheng ZY, Beuerman RW, Teoh SH, Zhu X, Tan DT. The development of a serum-free derived bioengineered conjunctival epithelial equivalent using an ultrathin poly (caprolactone) membrane substrate. Invest Ophthalmol Vis Sci 2006; 47:105–12.
54. Sharma S, Mohanty S, Gupta D, Jassal M, Agrawal AK, Tandon R. Cellular response of limbal epithelial cells on electrospun poly-ε-caprolactone nanofibrous scaffolds for ocular surface bioengineering: a preliminary in vitro study. Mol Vis. 2011; 17:2898-910.
55. Zhang H, Chia-Ying L, Hollister SJ. The interaction between bone marrow stromal cells and RGD-modified three-dimensional porous polycaprolactone scaffolds. Biomaterials 2009; 30:4063–9.
56. Schermer A, Galvin S, Sun TT. Differentiation-related expression of a major 64K corneal keratin in vivo and in culture suggests limbal location of corneal epithelial stem cells. J Cell Biol 1986; 103: 49-62.
57. Kurpakus MA, Maniaci MT, Esco M. Expression of keratins K12, K4 and K14 during development of ocular surface epithelium. Curr Eye Res 1994; 13:805-14.
58. Chen Z, de Paiva CS, Luo L, Kretzer FL, Pflugfelder SC, Li DQ. Characterization of putative stem cell phenotype in human limbal epithelia. Stem Cells 2004; 22: 355-66.
59. Dong, M. Roos, T. Gruigters, P. Donaldson, S. Bullivant, et al., Differential expression of two gap junction proteins in corneal epithelium. Eur. J. Cell Biol 1994; 64:95–100.
60. A. Li, P.J. Simmons, P. Kaur. Identification and isolation of candidate human keratinocyte stem cells based on cell surface phenotype. Proc. Natl. Acad. Sci. USA. 1998; 95: 3902–07
61. Hayashi, K.R. Kenyon. Increased cytochrome oxidase activity in alkali-burned corneas. Curr. Eye Res 1998; 7:131–8.
62. Pajoohesh-Ganji A, Pal-Ghosh S, Simmens SJ, Stepp MA. Integrins in slow-cycling corneal epithelial cells at the limbus in the mouse. Stem Cells 2006; 24:1075-86.
63. Lütjen-Drecoll, P. Steuhl, W.H. Arnold. Morphologische Besonderheiten der Conjunctiva bulbi R. Marquardt (Ed.), Chronische Conjunctivitis – Trockenes Auge, Springer, Berlin. 1982; 25–34.
64. Steuhl, H.-J. Thiel. Histochemical and morphological study of the regenerating corneal epithelium after limbus to limbus denudation. Graefes Arch. Clin. Exp. Ophthalmol 1987; 225:53–58.
65. B. Lauweryns, J.J. van den Oord, L. Missotten. The transitional zone between limbus and peripheral cornea. An immunohistochemical study. Invest. Ophthalmol. Vis. Sci 1993; 34:1991–99
66. G. Pellegrini, E. Dellambra, O. Golisano, E. Martinelli, I. Fantozzi, S. Bondanza, D. Ponzin, F. McKeon, M. de Luca. p63 identifies keratinocyte stem cells. Proc. Natl. Acad. Sci. USA. 2001; 98; 3156–61.
67. Di Iorio E, Barbaro V, Ruzza A, Ponzin D, Pellegrini G, De Luca M. Isoforms of DeltaNp63 and the migration of ocular limbal cells in human corneal regeneration. Proc Natl Acad Sci 2005; 102:9523-8.
68. de Paiva CS, Chen Z, Corrales RM, Pflugfelder SC, Li DQ. ABCG2 transporter identifies a population of clonogenic human limbal epithelial cells. Stem Cells 2005; 23:63-73.
69. Raji B, Dansault A, Leemput J, de la Houssaye G, Vieira V, et al., The RNA-binding protein Musashi-1 is produced in the developing and adult mouse eye. Mol Vis. 2007; 13:1412-27.
70. Barbaro V, Testa A, Di Iorio E, Mavilio F, Pellegrini G, De Luca M. C/EBPdelta regulates cell cycle and self-renewal of human limbal stem cells. J Cell Biol 2007; 18:1037-49.
Recent Advances Tandon R et al
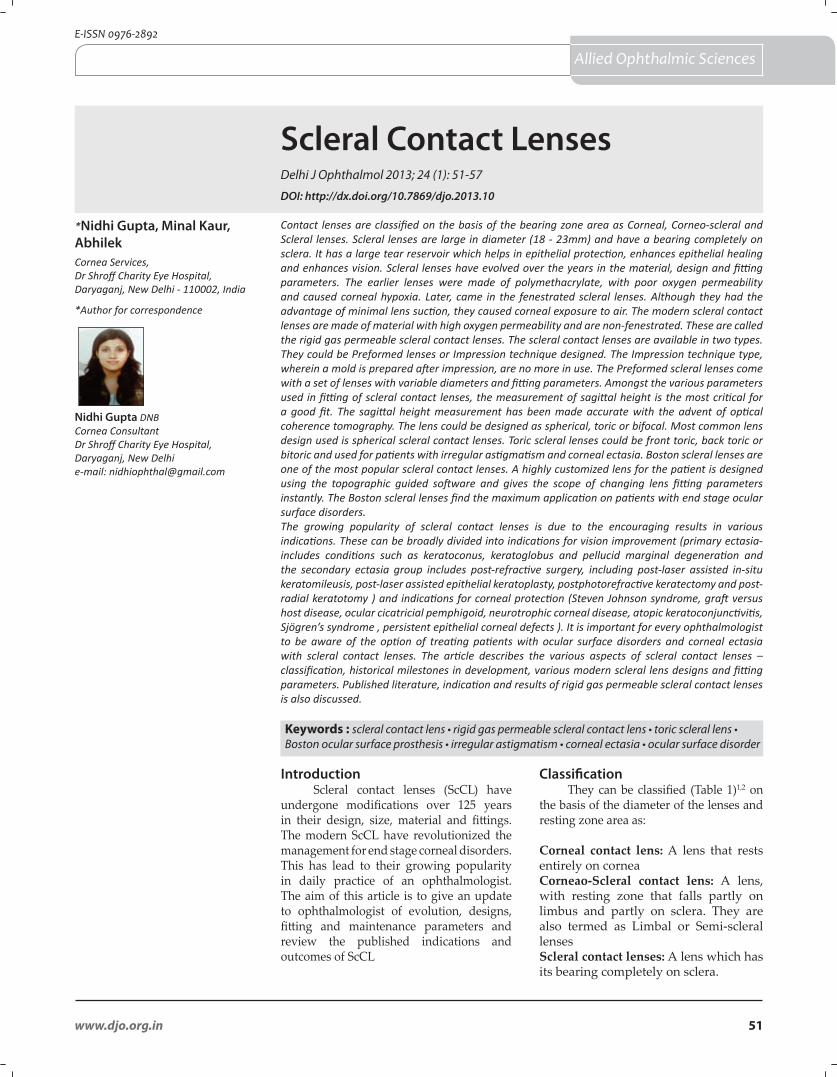
Scleral Contact LensesDelhi J Ophthalmol 2013; 24 (1): 51-57
Contact lenses are classified on the basis of the bearing zone area as Corneal, Corneo-scleral and Scleral lenses. Scleral lenses are large in diameter (18 - 23mm) and have a bearing completely on sclera. It has a large tear reservoir which helps in epithelial protection, enhances epithelial healing and enhances vision. Scleral lenses have evolved over the years in the material, design and fitting parameters. The earlier lenses were made of polymethacrylate, with poor oxygen permeability and caused corneal hypoxia. Later, came in the fenestrated scleral lenses. Although they had the advantage of minimal lens suction, they caused corneal exposure to air. The modern scleral contact lenses are made of material with high oxygen permeability and are non-fenestrated. These are called the rigid gas permeable scleral contact lenses. The scleral contact lenses are available in two types. They could be Preformed lenses or Impression technique designed. The Impression technique type, wherein a mold is prepared after impression, are no more in use. The Preformed scleral lenses come with a set of lenses with variable diameters and fitting parameters. Amongst the various parameters used in fitting of scleral contact lenses, the measurement of sagittal height is the most critical for a good fit. The sagittal height measurement has been made accurate with the advent of optical coherence tomography. The lens could be designed as spherical, toric or bifocal. Most common lens design used is spherical scleral contact lenses. Toric scleral lenses could be front toric, back toric or bitoric and used for patients with irregular astigmatism and corneal ectasia. Boston scleral lenses are one of the most popular scleral contact lenses. A highly customized lens for the patient is designed using the topographic guided software and gives the scope of changing lens fitting parameters instantly. The Boston scleral lenses find the maximum application on patients with end stage ocular surface disorders.The growing popularity of scleral contact lenses is due to the encouraging results in various indications. These can be broadly divided into indications for vision improvement (primary ectasia- includes conditions such as keratoconus, keratoglobus and pellucid marginal degeneration and the secondary ectasia group includes post-refractive surgery, including post-laser assisted in-situ keratomileusis, post-laser assisted epithelial keratoplasty, postphotorefractive keratectomy and post-radial keratotomy ) and indications for corneal protection (Steven Johnson syndrome, graft versus host disease, ocular cicatricial pemphigoid, neurotrophic corneal disease, atopic keratoconjunctivitis, Sjögren’s syndrome , persistent epithelial corneal defects ). It is important for every ophthalmologist to be aware of the option of treating patients with ocular surface disorders and corneal ectasia with scleral contact lenses. The article describes the various aspects of scleral contact lenses –classification, historical milestones in development, various modern scleral lens designs and fitting parameters. Published literature, indication and results of rigid gas permeable scleral contact lenses is also discussed.
*Nidhi Gupta, Minal Kaur, AbhilekCornea Services, Dr Shroff Charity Eye Hospital, Daryaganj, New Delhi - 110002, India
*Author for correspondence
Introduction Scleral contact lenses (ScCL) have
undergone modifications over 125 years in their design, size, material and fittings. The modern ScCL have revolutionized the management for end stage corneal disorders. This has lead to their growing popularity in daily practice of an ophthalmologist. The aim of this article is to give an update to ophthalmologist of evolution, designs, fitting and maintenance parameters and review the published indications and outcomes of ScCL
Classification They can be classified (Table 1)1,2 on
the basis of the diameter of the lenses and resting zone area as:
Corneal contact lens: A lens that rests entirely on corneaCorneao-Scleral contact lens: A lens, with resting zone that falls partly on limbus and partly on sclera. They are also termed as Limbal or Semi-scleral lensesScleral contact lenses: A lens which has its bearing completely on sclera.
Keywords : scleral contact lens • rigid gas permeable scleral contact lens • toric scleral lens • Boston ocular surface prosthesis • irregular astigmatism • corneal ectasia • ocular surface disorder
Nidhi Gupta DNBCornea ConsultantDr Shroff Charity Eye Hospital, Daryaganj, New Delhie-mail: [email protected]
51www.djo.org.in
E-ISSN 0976-2892
Allied Ophthalmic Sciences
DOI: http://dx.doi.org/10.7869/djo.2013.10
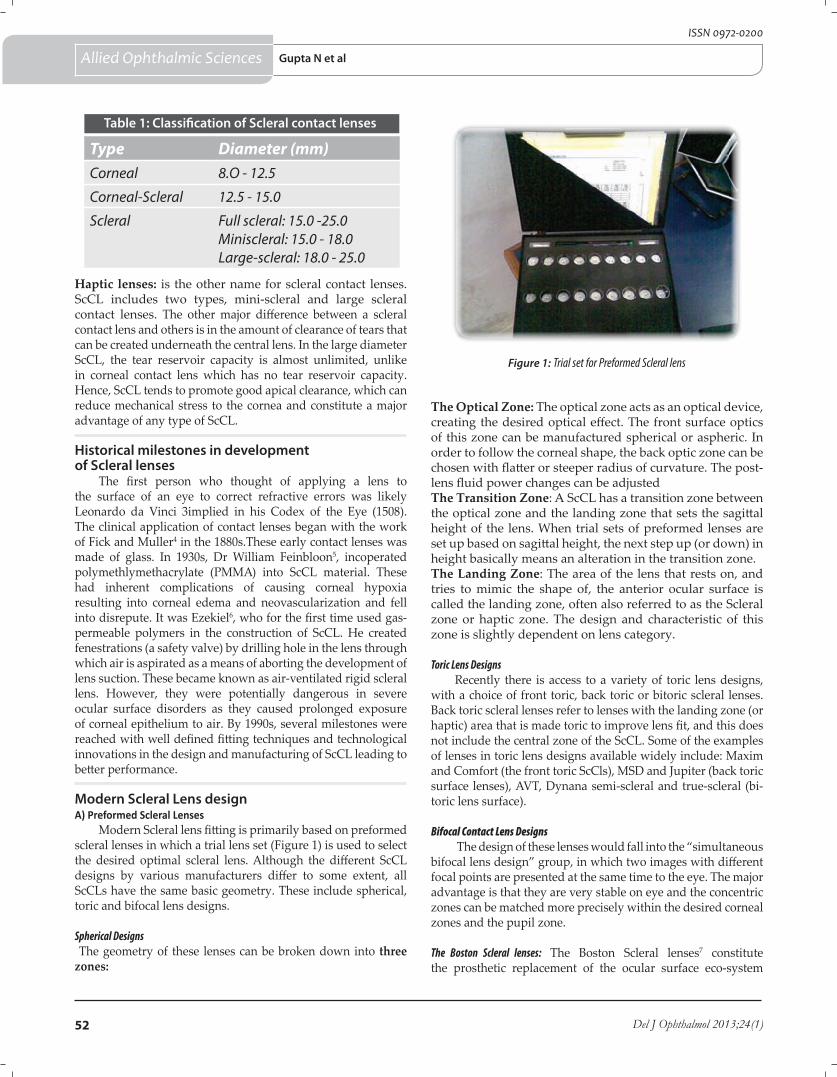
Haptic lenses: is the other name for scleral contact lenses. ScCL includes two types, mini-scleral and large scleral contact lenses. The other major difference between a scleral contact lens and others is in the amount of clearance of tears that can be created underneath the central lens. In the large diameter ScCL, the tear reservoir capacity is almost unlimited, unlike in corneal contact lens which has no tear reservoir capacity. Hence, ScCL tends to promote good apical clearance, which can reduce mechanical stress to the cornea and constitute a major advantage of any type of ScCL.
Historical milestones in development of Scleral lenses
The first person who thought of applying a lens to the surface of an eye to correct refractive errors was likely Leonardo da Vinci 3implied in his Codex of the Eye (1508). The clinical application of contact lenses began with the work of Fick and Muller4 in the 1880s.These early contact lenses was made of glass. In 1930s, Dr William Feinbloon5, incoperated polymethlymethacrylate (PMMA) into ScCL material. These had inherent complications of causing corneal hypoxia resulting into corneal edema and neovascularization and fell into disrepute. It was Ezekiel6, who for the first time used gas-permeable polymers in the construction of ScCL. He created fenestrations (a safety valve) by drilling hole in the lens through which air is aspirated as a means of aborting the development of lens suction. These became known as air-ventilated rigid scleral lens. However, they were potentially dangerous in severe ocular surface disorders as they caused prolonged exposure of corneal epithelium to air. By 1990s, several milestones were reached with well defined fitting techniques and technological innovations in the design and manufacturing of ScCL leading to better performance.
Modern Scleral Lens designA) Preformed Scleral Lenses
Modern Scleral lens fitting is primarily based on preformed scleral lenses in which a trial lens set (Figure 1) is used to select the desired optimal scleral lens. Although the different ScCL designs by various manufacturers differ to some extent, all ScCLs have the same basic geometry. These include spherical, toric and bifocal lens designs.
Spherical Designs The geometry of these lenses can be broken down into three zones:
The Optical Zone: The optical zone acts as an optical device, creating the desired optical effect. The front surface optics of this zone can be manufactured spherical or aspheric. In order to follow the corneal shape, the back optic zone can be chosen with flatter or steeper radius of curvature. The post-lens fluid power changes can be adjusted The Transition Zone: A ScCL has a transition zone between the optical zone and the landing zone that sets the sagittal height of the lens. When trial sets of preformed lenses are set up based on sagittal height, the next step up (or down) in height basically means an alteration in the transition zone. The Landing Zone: The area of the lens that rests on, and tries to mimic the shape of, the anterior ocular surface is called the landing zone, often also referred to as the Scleral zone or haptic zone. The design and characteristic of this zone is slightly dependent on lens category.
Toric Lens DesignsRecently there is access to a variety of toric lens designs,
with a choice of front toric, back toric or bitoric scleral lenses. Back toric scleral lenses refer to lenses with the landing zone (or haptic) area that is made toric to improve lens fit, and this does not include the central zone of the ScCL. Some of the examples of lenses in toric lens designs available widely include: Maxim and Comfort (the front toric ScCls), MSD and Jupiter (back toric surface lenses), AVT, Dynana semi-scleral and true-scleral (bi-toric lens surface).
Bifocal Contact Lens Designs The design of these lenses would fall into the “simultaneous
bifocal lens design” group, in which two images with different focal points are presented at the same time to the eye. The major advantage is that they are very stable on eye and the concentric zones can be matched more precisely within the desired corneal zones and the pupil zone.
The Boston Scleral lenses: The Boston Scleral lenses7 constitute the prosthetic replacement of the ocular surface eco-system
Figure 1: Trial set for Preformed Scleral lens
Type Diameter (mm)Corneal 8.O - 12.5
Corneal-Scleral 12.5 - 15.0
Scleral Full scleral: 15.0 -25.0Miniscleral: 15.0 - 18.0Large-scleral: 18.0 - 25.0
Table 1: Classification of Scleral contact lenses
52 Del J Ophthalmol 2013;24(1)
Gupta N et al Allied Ophthalmic Sciences
ISSN 0972-0200

(PROSE), which is the treatment model developed by the Boston Foundation for Sight (BFS) (Needham, MA) to restore vision, support healing, reduce symptoms and improve quality of life for patients suffering with complex corneal diseases. It was approved by Federal drug administration in 1994. The prosthetic device is made from an oversized button of itafluorocon B(Equalens II),a fluro-silicon/acrylate polymer of Dk value 87 x10-11 units. Each device is highly customized in its design and fabrication to address the circumstances and needs of the eyes ocular surface. This is done by using proprietary computer-assisted design and manufacture (CAD/CAM) software that is linked to a manufacturing lathe. It helps to achieve a satisfactory fit by designing the posterior surface and residual refractive error is incorporated into the frontal optical surface of the device.
B) Impression Technique Scleral LensesImpression techniques have been utilized successfully for
many years8, although not very commonly used in modern contact lens practice. With this technique, a mold is made of the anterior ocular surface (the positive cast), which is sent to a specialized manufacturer to produce a ScCL. These lenses follow the shape of the anterior surface precisely, and the impression retains its shape indefinitely so the lens can be reproduced at a later time. The downside of these lenses is that heat is required, which makes this technique basically limited to PMMA materials. Furthermore, preformed ScCL can be made thinner than molded lenses. Also, preformed lenses are more reproducible because the precise lens specifications are known and the lenses are easier to adjust. New technology such as OCT9,10 as described earlier, to image the anterior ocular shape could potentially lead to a revival of these custom made lenses without having to make the invasive molds and casts, which can then be manufactured in the highest Dk materials available.
Material of sclera contact lenses
ScCLs are considerably thicker than normal Gas Permeable lenses. It can be 0.4 to 0.6 mm in thickness, which can dramatically decrease the effective Dk/t of the lenses. The lenses are made out of special buttons with a diameter of up to 26 mm. They are made of high–oxygen permeable polymer material with Dk of 100 or more. The oxygen permeability of the lens allows oxygen to pass through the lens. Tear flow underneath the lens, if present, can also bring in oxygen-rich tears to supplement the oxygen demand of the cornea. Since typically the lens vaults the limbus in scleral lenses, oxygen from the conjunctival and limbal vessels can also contribute to the oxygen supply in the fluid layer.
Fitting and MaintenanceScCL are primarily fitted based on sagittal depth. Sagittal
height or apical height of a lens is the distance between a flat surface and the back surface of the central portion of the lens. It is dependent on a number of variables including lens diameter, radius of curvature, asphericity of the cornea, and the shape of the anterior sclera. Only with advanced topographical technology such as the OCT9 can the total sagittal height of the
anterior eye be measured. But by using a fitting set, the anterior surface topography can be empirically met in a clinically proven, successful way. Scleral lenses should have enough total diameters to bear the weight of the entire lens on the anterior ocular surface and to create a sufficient tear reservoir. Creating adequate corneal clearance is the key advantage in Scleral lens fitting To respect the shape of the anterior surface, aligning the landing zone with the anterior ocular surface and creating adequate edge lift is important .ScCL can be cleaned using approved Gas Permeable lens cleaning and disinfecting products or off-label use of multipurpose soft lens solutions. Prescribing a hydrogen peroxide-based care system eliminates exposure to any potential toxins or antigens.
Indications1. Vision Improvement
Correcting the irregular cornea to restore vision is the main indication for fitting ScCLs. The largest segment in this category is corneal ectasia11-16, which can be subdivided into two groups. First is the Primary corneal ectasia group, which includes conditions such as keratoconus, keratoglobus and pellucid marginal degeneration. The Secondary ectasia group includes post-refractive surgery, including post-laser assisted in-situ keratomileusis (LASIK), post-laser assisted epithelial keratoplasty (LASEK), postphotorefractive keratectomy (PRK) and post-radial keratotomy (RK), and trauma. Post keratoplasty astigmatism and eyes with significant scarring and severely irregular corneas due to trauma can achieve excellent vision with ScCL. Corneal degenerations or dystrophies, such as Terrien’s marginal degeneration (Figure2 & 3)and Salzmann’s nodular degeneration, are also indications.
2. Corneal ProtectionMain indication is ocular surface diseases17-21 such as
Steven’s Johnson Syndrome (Figure 4 & 5), Graft Versus Host Disease (Figure 6 & 7), ocular cicatricial pemphigoid, neurotrophic corneal disease and atopic keratoconjunctivitis, Sjögren’s syndrome , persistent epithelial corneal defects. Also, if lid closure is incomplete such as in eyelid coloboma, exophthalmus, ectropion, nerve palsies and after lid retraction surgery , a ScCL may be a good indication. In addition: in cases of trichiasis and entropion, ScCLs have shown to be effective in protecting the ocular surface. In symblepharon, a ScCL can act as a device to maintain the fornix, for instance after chemical burn.3. Recent indications
More recently, ScCLs have also been applied to deliver pharmaceuticals to the anterior surface for different reasons. One such indication is the application of antibiotics while the ocular surface recovers/heals, such as the treatment of persistent corneal epithelial defects with the ScCLs and an antibiotic adjunct.
Scleral Contact Lenses : Clinical Outcomes
The published literature on scleral contact lenses is summarised in (Table 2). The study on ScCL by Tan et al11 at Singapore eye hospital was one of the earliest for modern
53www.djo.org.in
Scleral contact lenses Allied Ophthalmic Sciences
E-ISSN 0976-2892
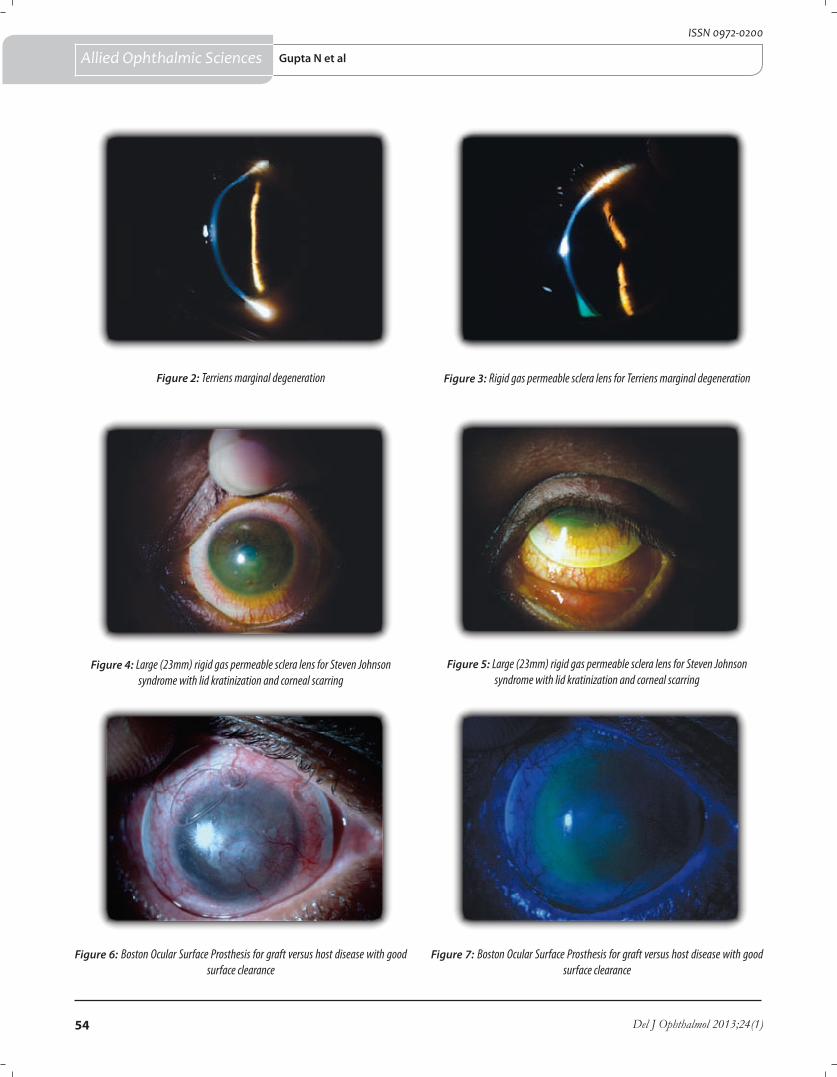
Figure 6: Boston Ocular Surface Prosthesis for graft versus host disease with good surface clearance
Figure 7: Boston Ocular Surface Prosthesis for graft versus host disease with good surface clearance
54 Del J Ophthalmol 2013;24(1)
Allied Ophthalmic Sciences
Figure 2: Terriens marginal degeneration Figure 3: Rigid gas permeable sclera lens for Terriens marginal degeneration
Figure 4: Large (23mm) rigid gas permeable sclera lens for Steven Johnson syndrome with lid kratinization and corneal scarring
Figure 5: Large (23mm) rigid gas permeable sclera lens for Steven Johnson syndrome with lid kratinization and corneal scarring
ISSN 0972-0200
Gupta N et al
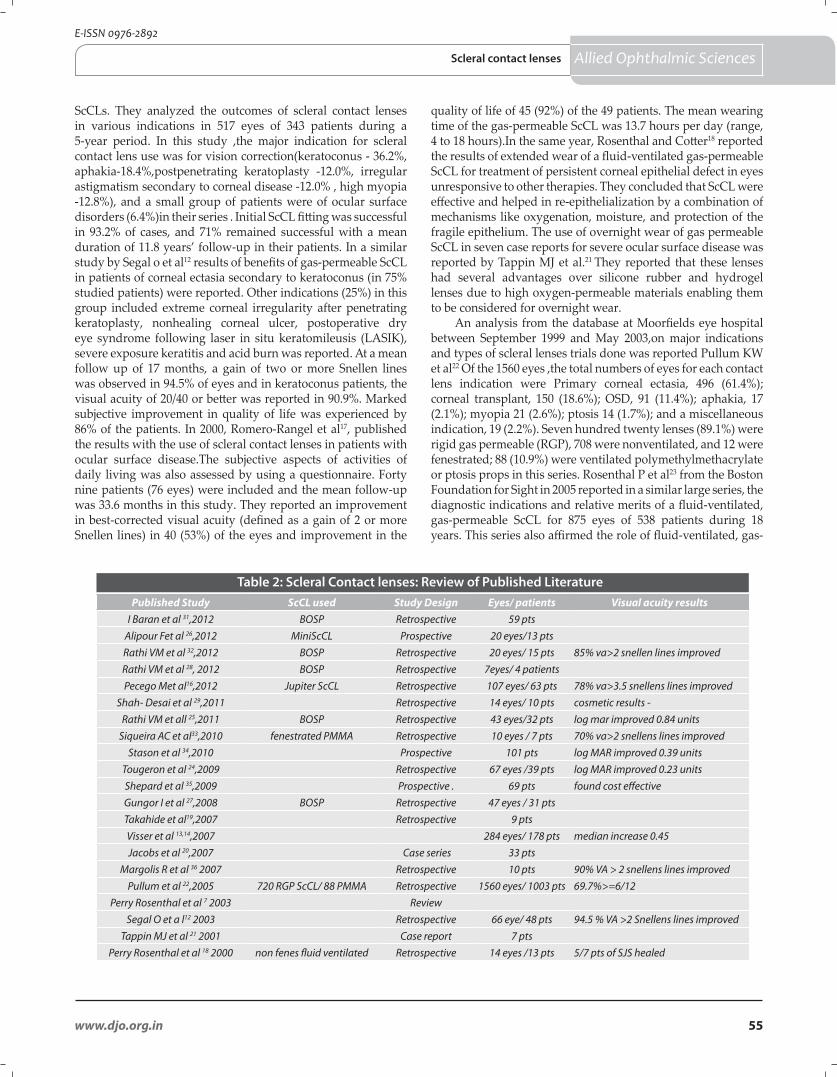
ScCLs. They analyzed the outcomes of scleral contact lenses in various indications in 517 eyes of 343 patients during a 5-year period. In this study ,the major indication for scleral contact lens use was for vision correction(keratoconus - 36.2%, aphakia-18.4%,postpenetrating keratoplasty -12.0%, irregular astigmatism secondary to corneal disease -12.0% , high myopia -12.8%), and a small group of patients were of ocular surface disorders (6.4%)in their series . Initial ScCL fitting was successful in 93.2% of cases, and 71% remained successful with a mean duration of 11.8 years’ follow-up in their patients. In a similar study by Segal o et al12 results of benefits of gas-permeable ScCL in patients of corneal ectasia secondary to keratoconus (in 75% studied patients) were reported. Other indications (25%) in this group included extreme corneal irregularity after penetrating keratoplasty, nonhealing corneal ulcer, postoperative dry eye syndrome following laser in situ keratomileusis (LASIK), severe exposure keratitis and acid burn was reported. At a mean follow up of 17 months, a gain of two or more Snellen lines was observed in 94.5% of eyes and in keratoconus patients, the visual acuity of 20/40 or better was reported in 90.9%. Marked subjective improvement in quality of life was experienced by 86% of the patients. In 2000, Romero-Rangel et al17, published the results with the use of scleral contact lenses in patients with ocular surface disease.The subjective aspects of activities of daily living was also assessed by using a questionnaire. Forty nine patients (76 eyes) were included and the mean follow-up was 33.6 months in this study. They reported an improvement in best-corrected visual acuity (defined as a gain of 2 or more Snellen lines) in 40 (53%) of the eyes and improvement in the
quality of life of 45 (92%) of the 49 patients. The mean wearing time of the gas-permeable ScCL was 13.7 hours per day (range, 4 to 18 hours).In the same year, Rosenthal and Cotter18 reported the results of extended wear of a fluid-ventilated gas-permeable ScCL for treatment of persistent corneal epithelial defect in eyes unresponsive to other therapies. They concluded that ScCL were effective and helped in re-epithelialization by a combination of mechanisms like oxygenation, moisture, and protection of the fragile epithelium. The use of overnight wear of gas permeable ScCL in seven case reports for severe ocular surface disease was reported by Tappin MJ et al.21 They reported that these lenses had several advantages over silicone rubber and hydrogel lenses due to high oxygen-permeable materials enabling them to be considered for overnight wear.
An analysis from the database at Moorfields eye hospital between September 1999 and May 2003,on major indications and types of scleral lenses trials done was reported Pullum KW et al22 Of the 1560 eyes ,the total numbers of eyes for each contact lens indication were Primary corneal ectasia, 496 (61.4%); corneal transplant, 150 (18.6%); OSD, 91 (11.4%); aphakia, 17 (2.1%); myopia 21 (2.6%); ptosis 14 (1.7%); and a miscellaneous indication, 19 (2.2%). Seven hundred twenty lenses (89.1%) were rigid gas permeable (RGP), 708 were nonventilated, and 12 were fenestrated; 88 (10.9%) were ventilated polymethylmethacrylate or ptosis props in this series. Rosenthal P et al23 from the Boston Foundation for Sight in 2005 reported in a similar large series, the diagnostic indications and relative merits of a fluid-ventilated, gas-permeable ScCL for 875 eyes of 538 patients during 18 years. This series also affirmed the role of fluid-ventilated, gas-
Published Study ScCL used Study Design Eyes/ patients Visual acuity resultsI Baran et al 31,2012 BOSP Retrospective 59 pts
Alipour Fet al 26,2012 MiniScCL Prospective 20 eyes/13 ptsRathi VM et al 32,2012 BOSP Retrospective 20 eyes/ 15 pts 85% va>2 snellen lines improvedRathi VM et al 28, 2012 BOSP Retrospective 7eyes/ 4 patientsPecego Met al16,2012 Jupiter ScCL Retrospective 107 eyes/ 63 pts 78% va>3.5 snellens lines improved
Shah- Desai et al 29,2011 Retrospective 14 eyes/ 10 pts cosmetic results -Rathi VM et all 25,2011 BOSP Retrospective 43 eyes/32 pts log mar improved 0.84 units
Siqueira AC et al33,2010 fenestrated PMMA Retrospective 10 eyes / 7 pts 70% va>2 snellens lines improvedStason et al 34,2010 Prospective 101 pts log MAR improved 0.39 units
Tougeron et al 24,2009 Retrospective 67 eyes /39 pts log MAR improved 0.23 unitsShepard et al 35,2009 Prospective . 69 pts found cost effective Gungor I et al 27,2008 BOSP Retrospective 47 eyes / 31 ptsTakahide et al19,2007 Retrospective 9 ptsVisser et al 13,14,2007 284 eyes/ 178 pts median increase 0.45Jacobs et al 20,2007 Case series 33 pts
Margolis R et al 36 2007 Retrospective 10 pts 90% VA > 2 snellens lines improvedPullum et al 22,2005 720 RGP ScCL/ 88 PMMA Retrospective 1560 eyes/ 1003 pts 69.7%>=6/12
Perry Rosenthal et al 7 2003 ReviewSegal O et a l12 2003 Retrospective 66 eye/ 48 pts 94.5 % VA >2 Snellens lines improved
Tappin MJ et al 21 2001 Case report 7 ptsPerry Rosenthal et al 18 2000 non fenes fluid ventilated Retrospective 14 eyes /13 pts 5/7 pts of SJS healed
Table 2: Scleral Contact lenses: Review of Published Literature
55www.djo.org.in
Allied Ophthalmic Sciences
E-ISSN 0976-2892
Scleral contact lenses

permeable scleral lens as a front-line tool for management of many corneal disorders refractory to other treatment measures.
The results of toric scleral lenses were reported by Visser ES et al13 in their cross-sectional survey, results with four types of ScCL primarily in keratoconus patients. The study was done with lenses which were cut by precise Sub Micron Lathing from a Boston Equalens II blank at Procornea. They included spherical, front-surface toric, back-surface toric, and bitoric lens designs. Results revealed a sharp increase in visual acuity after toric lens use in this study. Visser ES et al14 al also evaluated the subjective performance of the toric lenses. The subjective performance was investigated during an interview that included the use of a five-point Likert scale and by means of a questionnaire supplemented by a 100-mm visual analog scale (VAS). High patient satisfaction was seen in all patients and the back-surface toric designs s compared to the back-surface spherical designs showed better results. The beneficial results of Jupiter Scleral contact lenses with back toric lens design (Medlens Innovations,Front Royal, VA; and Essilor Contact Lenses, Inc., Dallas, TX) in the management of 32 patients of keratoconus was reported by Schornack MMet al15. Pecego M et al 16, evaluated results of fitting the Jupiter Scleral Lens in 63 patients (107 eyes) with major indication being keratoconus. The improvement in best-corrected visual acuity compared with previous contact lens or glasses correction was a mean gain of 3.5 Snellen lines.
Takahide K et al19 reported outcomes of scleral contact lenses in 9 patients of cGVHD-related severe Keratoconjunctivitis sicca that was refractory to standard treatments. All patients in this series reported improvement of ocular symptoms and reduced use of topical lubricants after ScCL fitting resulting from decreased evaporation. Jacob DS et al20 reported results with the Boston ScCL Prosthetic Device (BSLPD) in similar group of patients with severe dry eye from chronic graft-versus-host disease in 33 patients. The results of BSLD in these patients showed that more than half had the highest improvement level for pain (52%) and photophobia (63%), and more than two thirds (73%) had the highest improvement level for quality of life. There was improvement in reading and driving in >90% of those who reported previous compromise, with >60% reporting the highest improvement level for each of these activities. Tougeron-Brousseau B et al24, described the therapeutic benefits of ScCL in the management of severe ocular surface disease attributable to toxic epidermal necrolysis (TEN) and Stevens-Johnson syndrome (SJS) in 39 patients (67 eyes). The main outcome measures in this study were best-corrected visual acuity (VA) and OSDI and NEI VFQ-25 composite score before and 6 months after Scleral contact lens fitting. In this series results showed , Visual acuity in the better eye (36 patients, 36 eyes) progressed from 0.73 to 0.50 logarithm of the minimum angle of resolution (P = .0001) 6 months after ScCL placement in patients fitted with lenses. The mean OSDI improved from 76.9 +/- 22.8 to 37.1 +/- 26.7 (P =.0001). Thirty-two NEI VFQ-25 composite scores were available. The mean NEIVFQ-25 composite score reportedly improved from 25.1 +/- 16.8 to 67.4 +/- 22.1 (P = .0001) Rathi et al25, reported utilization of Boston Ocular Surface Prosthesis (BOSP) in 23 eyes of corneal ectasia
and 20eyes of Steven Johnsons Syndrome. There was a significant improvement in pre- and post-BOSP wear mean LogMAR Visual Acuity. ). A study by Alipour Fet al26 on mini-scleral contact lenses, for management of moderate to severe dry eye .They reported decrease in discomfort and dry eye symptoms, decrease artificial tear need frequency and improvement in visual acuity during mean follow up period of 18.25 months.
The results in peadiatric patients was reported by Gungor et al 27. They reported the use of a custom-designed, fluid-ventilated, gas-permeable ScCL in the treatment of patients less than 13 years of age in 47 eyes of 31 patients. A broad range of refractive and ocular surface disorders was treated with this modality, with the vast majority of patients having ocular surface disease (27/31, 87%) rather than refractive disorders (4/31, 13%). Rathi Vm28 et al studied the use of fluid-filled Scleral contact lenses in patients with vernal keratoconjunctivitis. They concluded that with coexisting keratoconus and VKC, ScCL improves vision and helps to maintain the health of the ocular surface. Shah-Desai SD et al29 studied the results of ScCL in patients of Ptosis. The study concluded that ScCLs provide a well-tolerated and practical long-term solution to safely elevating the upper eyelid in patients where complex ptosis is present. The patients were reportedly satisfied with the cosmetic appearance achieved.
Kalwerisky K et al30 reported the use of the BOSP in patients with severe periorbital thermal injuries in (16 eyes) who were treated for exposure keratopathy. Rehabilitation of the ocular surface was accomplished using the BOSP, with 10 of the 16 treated eyes achieving a corrected visual acuity of 20/70 or better in their study. Five eyes achieved a best-corrected visual acuity of 20/40 or better
ComplicationsThese include2,37,38 air bubbles behind the lens, bulbar
redness, conjunctival blanching and staining, corneal staining, Giant Papillary Conjunctivitis (GPC), hypoxia and edema, lens adhesion, neovascularization of cornea and graft microcystic edema. This requires lens exchange. Microbial keratitis and infiltrates in cornea have been reported in patients with steroid use or poor hygiene.
ConclusionGas permeable scleral contact lens has visual and
therapeutic benefits primarily in ocular surface disorders and corneal astigmatism in which conventional management fails. Advances in lens design and highly customized fit makes it a practical option for an increasing number and variety of patients with corneal disease. It is evolving into a lens useful in daily practice of clinicians treating these disorders. All ophthalmologists should be aware of scleral rigid gas-permeable lenses as a therapeutic option for their patients.
Financial & competing interest disclosureThe authors do not have any competing interests in any product /
procedure mentioned in this study. The authors do not have any financial interests in any product / procedure mentioned in this study
56 Del J Ophthalmol 2013;24(1)
Allied Ophthalmic Sciences
ISSN 0972-0200
Gupta N et al
57www.djo.org.in
References
1. DeNaeyer G .Reader and Industry Forum: A New Way to Classify Scleral Contact Lenses. Contact Lens Spectrum 2011; October:p-60.
2. Van der Worp E. A Guide to Scleral Lens Fitting. Scleral Lens Education Society 2010. Available at:http://commons.pacificu.edu/mono/4 .
3. da Vinci L.Codex of the eye, Manuscript D (circa 1508). Am J Optom 1953; 30:41-44.
4. Fick AE . In contractbrille. Arch Augenheilkd 1888; 17:215-26.5. Feinbloom WA. Plastic contact lenses. Am J Ophthalmol 1937;
14:41-9.6. Ezekiel D .Gas permeable haptic lenses. J Br Contact Lens Assoc
1983 ;6:158-61.7. Rosenthal P, Cotter J.The Boston Scleral Lens in the
management of severe ocular surface disease. Ophthalmol Clin North Am 2003; 16:89-93.
8. Pullum KW. Scleral contact lenses. In:Speedwell L, Phillips AJ,eds Contact Lenses. Oxford, UK, Elsevier, 2007, pp 333 – 353 .
9. Gemoules G .A novel method of fitting scleral lenses using high resolution optical coherence tomography. Eye Contact Lens 2008; 34:80-3.
10. Le HG, Tang M, Ridges R, Huang D, Jacobs DS. Pilot Study for OCT Guided Design and Fit of a Prosthetic Device for Treatment of Corneal Disease. J Ophthalmol 2012; 2012: 812430.
11. Tan DTH, Pullum KW, Buckley RJ. Medical applications of scleral contact lenses: A retrospective analysis of 343 cases.Cornea 1995; 14:121-9.
12. Segal O, Barkana Y, Hourovitz D, Behrman S, Kamun Y et al. Scleral contact lenses may help where other modalities fail. Cornea 2003; 22:308-10.
13. Visser ES, Visser R, van Lier HJ, Otten HM .Modern scleral lenses Part I. Clinical features. Eye and Contact Lens 2007; 33:13-20.
14. Visser ES, Visser R, van Lier HJ, Otten HM .Modern scleral lenses Part II. Patient satisfaction. Eye and Contact Lens 2007; 33: 21-5.
15. Schornack MM, Patel SV. Scleral lenses in the management of keratoconus. Ophthal Plast Reconstr Surg 2011; 27:95-8.
16. J Pecego M, Barnett M, Mannis MJ, Durbin-Johnson B. Jupiter Scleral Lenses: the UC Davis Eye Center experience. Eye Contact Lens 2012; 38:179-82.
17. Romero-Rangel T, Stavrou P, Cotter J, Rosenthal P, Baltatzis S, Foster CS. Gas-permeable scleral contact lens therapy in ocular surface disease. Am J Ophthalmol 2000; 130:25-32.
18. Rosenthal P, Cotter JM, Baum J .Treatment of persistent corneal epithelial defect with extended wear of a fluid-ventilated gas-permeable scleral contact lens. Am J Ophthalmol 2000; 130:33-41.
19. Takahide K, Parker PM, Wu M, Hwang WY, Carpenter PA, Moravec C et al .Use of fluid-ventilated, gas-permeable scleral lens for management of severe keratoconjunctivitis sicca secondary to chronic graft-versus-host disease. Biol Blood Marrow Transplant 2007; 13:1016-21.
20. Jacobs DS, Rosenthal P .Boston scleral lens prosthetic device for treatment of severe dry eye in chronic graft-versus-host disease. Cornea 2007; 26:1195-9.
21. Tappin MJ, Pullum KW, Buckley RJ .Scleral contact lenses for overnight wear in the management of ocular surface disorders. Eye 2001; 15:168-72.
22. Pullum KW, Whiting MA, Buckley RJ Scleral contact lenses: the expanding role. Cornea 2005; 24:269-77.
23. Rosenthal P, Croteau A. Fluid-ventilated, gas-permeable scleral contact lens is an effective option for managing severe ocular surface disease and many corneal disorders that would otherwise require penetrating keratoplasty. Eye Contact Lens 2005; 31:130-4.
24. Tougeron-Brousseau B, Delcampe A, Gueudry J, Vera L, Doan S, Hoang-Xuan etal. Vision-related function after scleral lens fitting in ocular complications of Stevens-Johnson syndrome and toxic epidermal necrolysis. Am J Ophthalmol 2009; 148:852-9.
25. Rathi VM, Mandathara PS, Dumpati S, Vaddavalli PK, Sangwan VS. Ophthalmology Boston ocular surface prosthesis: an Indian experience. Indian J Ophthalmol 2011; 59:279-81.
26. Alipour F, Kheirkhah A, Jabarvand Behrouz M.Use of mini scleral contact lenses in moderate to severe dry eye. Cont Lens Anterior Eye 201; 35:272-6.
27. Gungor I, Schor K, Rosenthal P, Jacobs DS. The Boston Scleral Lens in the treatment of pediatric patients. J AAPOS 2008; 12: 263-7.
28. Rathi VM, Sudharman Mandathara P, Vaddavalli PK, Dumpati S, Chakrabarti T,Sangwan VS. Fluid-filled scleral contact lenses in vernal keratoconjunctivitis. Cont Lens Anterior Eye 2012; 38: 203-6.
29. Shah-Desai SD, Aslam SA, Pullum K, Beaconsfield M, Rose GE .Scleral contact lens usage in patients with complex blepharoptosis. Indian J Ophthalmol 2011; 59:279-81.
30. Kalwerisky K, Davies B, Mihora L, Czyz CN, Foster JA, De Martelaere S .Use of the Boston Ocular Surface Prosthesis in the management of severe periorbital thermal injuries: a case series of 10 patients. Eye Contact Lens 2012; 38:203-6.
31. Baran I, Bradley JA, Alipour F, Rosenthal P, Le HG, Jacobs DS. PROSE treatment of corneal ectasia. Cont Lens Anterior Eye 2012; 35: 222-7.
32. Rathi VM, Mandathara PS, Vaddavalli PK, Srikanth D, Sangwan VS.Fluid filled scleral contact lens in pediatric patients: challenges and outcome. Cont Lens Anterior Eye 2012; 35: 189-92.
33. Siqueira AC, Santos MS, Farias CC, Barreiro TR, Gomes JÁ . Scleral contact lens for ocular rehabilitation in patients with Stevens-Johnson syndrome. Arq Bras Oftalmol 2010; 73:428-32.
34. Stason WB, Razavi M, Jacobs DS, Shepard DS, Suaya JA, Johns L, Rosenthal P. Clinical benefits of the Boston Ocular Surface Prosthesis. Am J Ophthalmol 2010 ;149:54-61.
35. Shepard DS, Razavi M, Stason WB, Jacobs DS, Cohen M, Rosenthal P. Economic appraisal of the Boston Ocular Surface Prosthesis. Am J Ophthalmol 2009; 148:860-8.
36. Margolis R, Thakrar V, Perez VL. Role of rigid gas-permeable scleral contact lenses in the management of advanced atopic keratoconjunctivitis. Cornea 2007; 26:1032-4.
37. Zimmerman AB, Marks A. Microbial Keratitis Secondary to Unintended Poor Compliance with Scleral Gas-Permeable Contact Lenses. Eye Contact Lens 2013. Feb 6.
38. Bruce AS, Nguyen LM. Acute red eye (non-ulcerative keratitis) associated with mini-scleral contact lens wear for keratoconus. Clin Exp Optom 2013; 9: 245-8.
Allied Ophthalmic Sciences
E-ISSN 0976-2892
Scleral contact lenses

58 Del J Ophthalmol 2013;24(1)
ISSN 0972-0200
Posterior ScleritisDelhi J Ophthalmol 2013; 24 (1): 58-60
Posterior scleritis is a relatively uncommon disorder and often misdiagnosed owing to its variable presentations. We describe two cases of posterior scleritis. Both the cases underwent a complete ophthalmic examination, fluorescein angiography, B-scan ultrasonography, systemic evaluation including physical examination and laboratory investigations. We did not find any associated systemic disease in our cases inspite of extensive investigations. Both the cases showed a good response to oral steroid in tapering dose. To detect the underlying disease, for proper treatment and assessment of prognosis, diagnostic work-up is needed. B-scan ultrasonography is the most useful diagnostic tool in such patients.Early diagnosis of posterior scleritis is important due to its excellent response to anti-inflammatory medication, particularly with systemic steroid and most common etiology being idiopathic.
*Chandana Chakraborti, Krittka Pal Chowdhury Dept of OphthalmologyCalcutta National Medical College & Hospital, Kolkata - 700006
*Author for correspondence
Introduction Scleritis can be identified as anterior
scleritis, posterior scleritis or episcleritis depending on the site of the inflammatory process within the scleral or episcleral tissue. Diagnosing anterior scleritis and episcleritis is much easier than diagnosing posterior scleritis because lesions can be more easily observed in the first two conditions. Posterior scleritis is probably one of the most underdiagnosed conditions in ophthalmology.1 It has diverse manifestations and can be easily overlooked. This diagnosis must be considered in all inflammatory and painful ocular disorders with no obvious etiology.2 We report two cases of posterior scleritis that were treated successfully with systemic steroid.
Case 1A-20 years old female presented on
20.11.2010 with complaints of pain, redness, watering and swelling of the left eye since two weeks. She was diagnosed as a case of acute viral conjunctivitis elsewhere and was prescribed topical antibiotics but the condition worsened. Incidentally an outbreak of epidemic viral conjunctivitis occurred in the city during the previous one month. Examination of left eye showed best corrected visual acuity (BCVA) 6/12, restricted ocular motility, conjunctival and episcleral congestion (Figure 1) and relative afferent pupillary defect (RAPD). Fundoscopy revealed disc oedema with multiple choroidal folds and a dull foveal reflex (Figure 2) , right eye was within normal limit. USG B- scan of left eye
showed characteristic ‘T-sign’ (Figure 3). Fundus Fluorescein Angiography (FFA) showed distended tortuous veins, disc oedema with leakage of dye in late frames on left eye (Figure 4). Routine blood, FBS, ACE, Rheumatoid (RA) factor, antinuclear antibodies (ANA), Antineutrophil cytoplasmic antibodies (ANCA), were all normal. ECG, chest X-Ray and X-Ray PNS revealed no abnormality. Her Mantoux test (Mx) was also within normal limits. Magnetic resonance imaging (MRI) showed thickening of left posterior sclera with thickened optic nerve (Figure 5).
She was diagnosed as a case of left anterior and posterior scleritis and started on oral steroid (60mg OD) therapy which was tapered over 6 weeks, along with topical nonsteroidal anti-inflammatory drugs. Marked improvement was found at 1 week follow up.
USG B- scan of left eye showed complete resolution at 1 month follow up. She developed similar attack in RE in January 2011 and in LE in April 2011 for which oral steroid was given for 6 weeks each time and the condition recovered. Patient was treated with alternate day 10mg prednisolone for one year and there is no recurrence till date.
Case 2 A middle age male presented with
the complaints of mild swelling, pain and dimness of vision in RE for 2 weeks, and a history of backache for the same duration. His BCVA was 6/12 (RE) and
Keywords : posterior scleritis • disc oedema • ‘T- sign’
Chandana Chakraborti MBBS, MD
Assistant Professor, Department of OphthalmologyA/1/1,Pearl Apartment, 50B, Kailas Bose Street, Kolkata 700006e mail - [email protected]
Photo Essay
DOI: http://dx.doi.org/10.7869/djo.2013.11
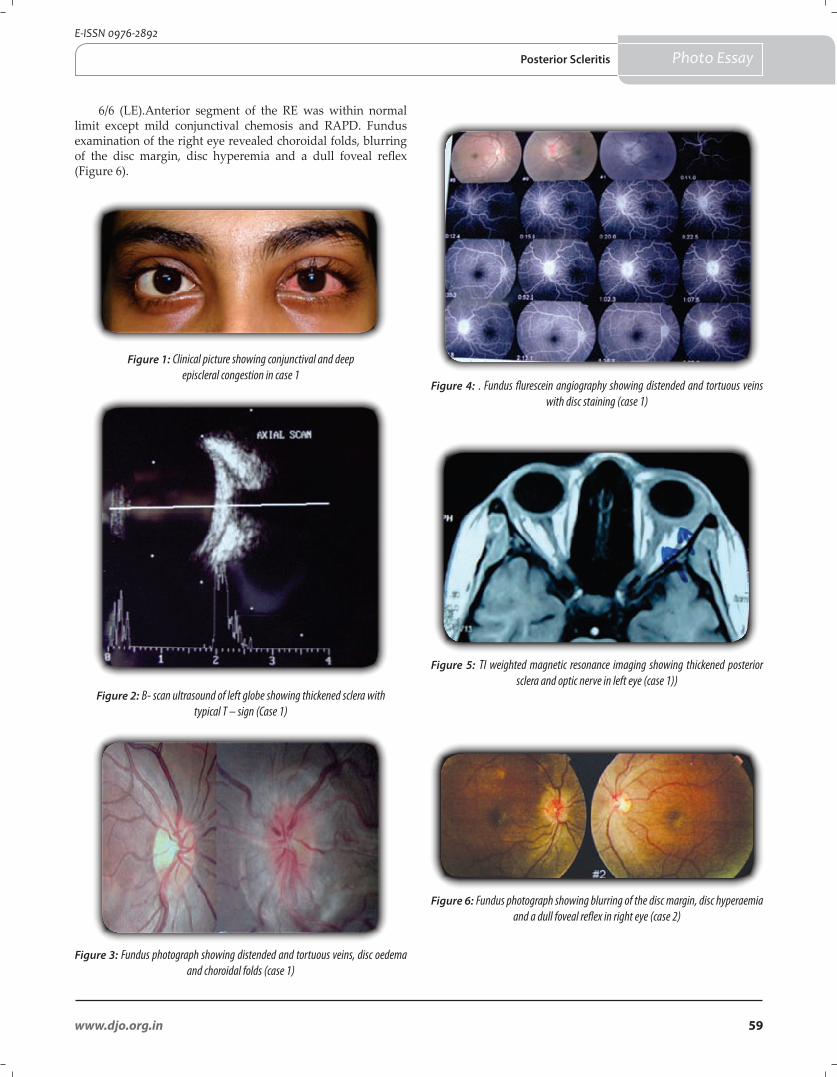
59www.djo.org.in
E-ISSN 0976-2892
6/6 (LE).Anterior segment of the RE was within normal limit except mild conjunctival chemosis and RAPD. Fundus examination of the right eye revealed choroidal folds, blurring of the disc margin, disc hyperemia and a dull foveal reflex (Figure 6).
Figure 1: Clinical picture showing conjunctival and deep episcleral congestion in case 1
Figure 2: B- scan ultrasound of left globe showing thickened sclera with typical T – sign (Case 1)
Figure 5: TI weighted magnetic resonance imaging showing thickened posterior sclera and optic nerve in left eye (case 1))
Figure 6: Fundus photograph showing blurring of the disc margin, disc hyperaemia and a dull foveal reflex in right eye (case 2)
Figure 4: . Fundus flurescein angiography showing distended and tortuous veins with disc staining (case 1)
Figure 3: Fundus photograph showing distended and tortuous veins, disc oedema and choroidal folds (case 1)
Photo EssayPosterior Scleritis

60 Del J Ophthalmol 2013;24(1)
ISSN 0972-0200
References
1. Watson PG. The nature and the treatment of scleral inflammation. Trans Ophthalmol Soc 1982; 102:257–281.
2. Ladjimi A, Messaoud R, Attia S, Jenzri S, Zaouali S, Chaouch K, Bhouri L et al.Posterior scleritis: six case reports. J Fr Ophtalmol 2003 ;26(8):845-52.
3. Akpek E K. Necrotizing scleritis: diagnosis and therapy. Ocular Immunology and Uveitis Foundation.www.uveitis.org/ last visited on 24.04.2013.
4. Foster CS, Sainz de la Maza M. The Sclera. Springer-Verlag, New York 1994, pp120-124.
5. Watson PG, Hayreh SS. Scleritis and episcleritis. Br J Ophthalmol 1976; 60:163-191.
6. McCluskey PJ,Watson PG, Lightman S, Haybittle J,Restori M, Brantley M. Posterior scleritis: clinical features, systemic associations, and outcome in a large series of patients. Ophthalmology 1999; 106:2380-6.
7. Nandi K, Sarkar S, Ranjan P, Biswas J. Posterior Scleritis: Clinical Profile and Visual Outcome in A Series of 32 Patients. AIOC 2009 Proceedings. 603-605. Available at : http://www.aios.org/proceed09/paper2009/UVEA/Uvea6.pdf .
8. Biswas J, Mittal S, Ganesh SK, Shetty NS, GopalL. Posterior Scleritis: clinical profile and imaging characteristics. Indian J Ophthalmol 1998; 46:195-2028.
9. Ohtsuka K, Hashimoto M, Miura M, Nakamura Y. Posterior scleritis with Optic perineuritis and internal ophthalmoplegia. Br J Ophthalmol 1997; 81:513.
10. Sainz de la Maza M, Foster CS, Jabbur NS. Scleritis associated with rheumatoid arthritis and with other systemic immune-mediated diseases. Ophthalmology 1994; 101:1281-6; discussion 1287-8.
11. Benson WE.Posterior scleritis. SurvOphthalmol 1988; 32:297-316.
No abnormality was detected in the left eye. Fasting and postprandial blood sugar, routine blood investigations were normal. Mx test was positive (18mm x 18mm). CRP and RA factor were within normal level. X-ray of chest and sacroili-ac joint showed no abnormality. USG B-Scan of the left eye showed characteristic ‘T- sign’. FFA revealed disc oedema, no leakage . On referral to Chest medicine tuberculosis was ruled out. He was treated as in like Case 1. Oral steroid was continued in tapering doses for 6 weeks. There has been no recurrence till date.
Discussion Scleritis is a severe inflammatory condition showing
microangiopathy in most of the specimens suggesting an underlying immune complex reaction. The antigen is usually the aberrant expression of the HLA-DR on scleral fibroblasts, induced by interferon gamma.3 Associated systemic diseases are Rheumatoid arthritis ,Wegener’s granulomatosis, SLE, JRA, PAN, Relapsing polychondritis, psoriasis, gout, atopy, rosacea, TB, syphilis, HSV, HZV.4,5 The average age in the largest series of posterior scleritis was 49.3 years with a female preponderance.6 Occurrence of posterior scleritis at a young age like in Case 1,though uncommon, has been reported in literature. Commonest presenting complaint among these patients is variable decrease of vision associated with moderate to severe ocular pain.7
As posterior scleritis patient may present with proptosis, lid swelling, limitation of ocular movements, one should consider orbital tumor, inflammatory pseudotumor or thyroid ophthalmopathy in the differential diagnosis. In case of subretinal mass findings, choroidal melanoma, metastatic uveal carcinoma, or choroidal hemangioma should be excluded. In cases with serous detachment of choroid, ciliary body or retina, conditions like uveal effusion syndrome, Vogt-Koyanagi-Harada disease or central serous retinopathy should be kept in mind.3,4
In one study idiopathic posterior scleritis was seen in 24 cases (75%), and there was an associated systemic disease in 8 patients (25%). In Case 1, both anterior and posterior sclera was involved. In earlier reports also the presence of anterior scleral involvement to variable extent has been seen commonly associated with posterior scleritis. Restriction of ocular movements can be seen with intense periscleral inflammation spreading to orbit and extraocular muscles.8 Disc oedema, choroidal folds, retinal detachments, subretinal mass lesions and elevated IOP are the commonest associations found in some studies.6,7 Low grade uveitis is uncommon in posterior scleritis.7 The condition may be associated with internal ophthalmoplegia caused by inflammatory damage to the cilliary ganglion and short ciliary nerves located around the optic nerve.9
Diagnostic tests like RA factor, ANA, ANCA, Eosinophil count, IgE, Uric acid, ESR ,Serological tests, Purified-protein derivative (PPD) skin test or Quantiferon gold assay, anergy skin test along with imaging studies of chest, sinus and sacroiliac joint may be considered as and when required. Ultrasonography (A- and B-scan) is the key investigation necessary to make the diagnosis of posterior scleritis. CT and MRI scans are especially
important in differential diagnosis of posterior scleritis or the diagnosis of the underlying disease.10 FFA show circumscribed fundus mass, choroidal folds, retinal striae, disc edema, annular choroidal detachment, exudative macular detachment, cystoid macular edema and localized peripheral retinal detachment.11
Corticosteroid should be the first line of therapy in this entity. Non-steroidal agents, oral steroids, and periocular steroids have been used successfully in the management of posterior scleritis. The disease usually shows a good response to systemic anti-inflammatory therapy. Complete resolution of inflammation often takes several weeks. Patients with loss of vision, evidence of optic nerve involvement, systemic disease needs aggressive anti inflammatory therapy with systemic immunosuppressive agents.6
Ophthalmologists must remain aware of the protean manifestations of this rare entity. Early diagnosis of posterior scleritis is important due to its excellent response to anti-inflammatory medication, particularly with systemic steroid.
Photo Essay Chakroborti & Chowdhury
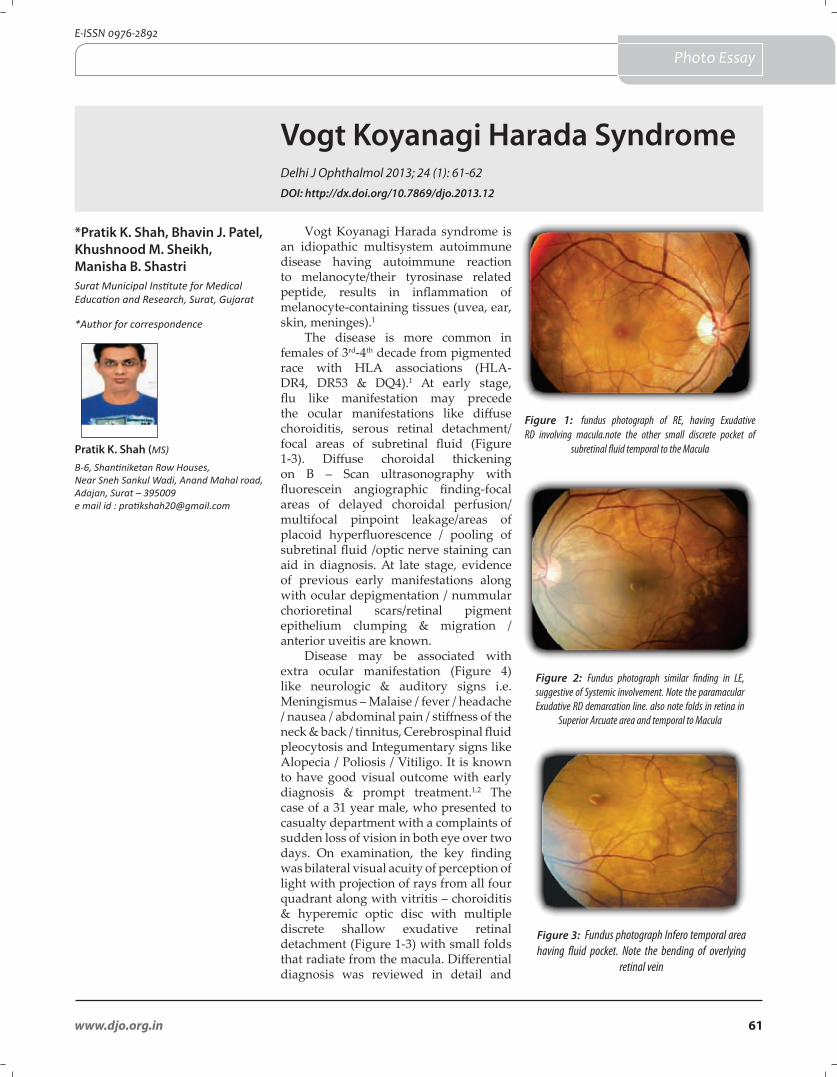
61www.djo.org.in
E-ISSN 0976-2892
Photo Essay
Vogt Koyanagi Harada SyndromeDelhi J Ophthalmol 2013; 24 (1): 61-62
*Pratik K. Shah, Bhavin J. Patel, Khushnood M. Sheikh, Manisha B. ShastriSurat Municipal Institute for Medical Education and Research, Surat, Gujarat
*Author for correspondence
Pratik K. Shah (MS)
B-6, Shantiniketan Row Houses,Near Sneh Sankul Wadi, Anand Mahal road,Adajan, Surat – 395009e mail id : [email protected]
Vogt Koyanagi Harada syndrome is an idiopathic multisystem autoimmune disease having autoimmune reaction to melanocyte/their tyrosinase related peptide, results in inflammation of melanocyte-containing tissues (uvea, ear, skin, meninges).1
The disease is more common in females of 3rd-4th decade from pigmented race with HLA associations (HLA-DR4, DR53 & DQ4).1 At early stage, flu like manifestation may precede the ocular manifestations like diffuse choroiditis, serous retinal detachment/focal areas of subretinal fluid (Figure 1-3). Diffuse choroidal thickening on B – Scan ultrasonography with fluorescein angiographic finding-focal areas of delayed choroidal perfusion/multifocal pinpoint leakage/areas of placoid hyperfluorescence / pooling of subretinal fluid /optic nerve staining can aid in diagnosis. At late stage, evidence of previous early manifestations along with ocular depigmentation / nummular chorioretinal scars/retinal pigment epithelium clumping & migration / anterior uveitis are known.
Disease may be associated with extra ocular manifestation (Figure 4) like neurologic & auditory signs i.e. Meningismus – Malaise / fever / headache / nausea / abdominal pain / stiffness of the neck & back / tinnitus, Cerebrospinal fluid pleocytosis and Integumentary signs like Alopecia / Poliosis / Vitiligo. It is known to have good visual outcome with early diagnosis & prompt treatment.1,2 The case of a 31 year male, who presented to casualty department with a complaints of sudden loss of vision in both eye over two days. On examination, the key finding was bilateral visual acuity of perception of light with projection of rays from all four quadrant along with vitritis – choroiditis & hyperemic optic disc with multiple discrete shallow exudative retinal detachment (Figure 1-3) with small folds that radiate from the macula. Differential diagnosis was reviewed in detail and
Figure 1: fundus photograph of RE, having Exudative RD involving macula.note the other small discrete pocket of
subretinal fluid temporal to the Macula
Figure 2: Fundus photograph similar finding in LE, suggestive of Systemic involvement. Note the paramacular Exudative RD demarcation line. also note folds in retina in
Superior Arcuate area and temporal to Macula
Figure 3: Fundus photograph Infero temporal area having fluid pocket. Note the bending of overlying
retinal vein
DOI: http://dx.doi.org/10.7869/djo.2013.12
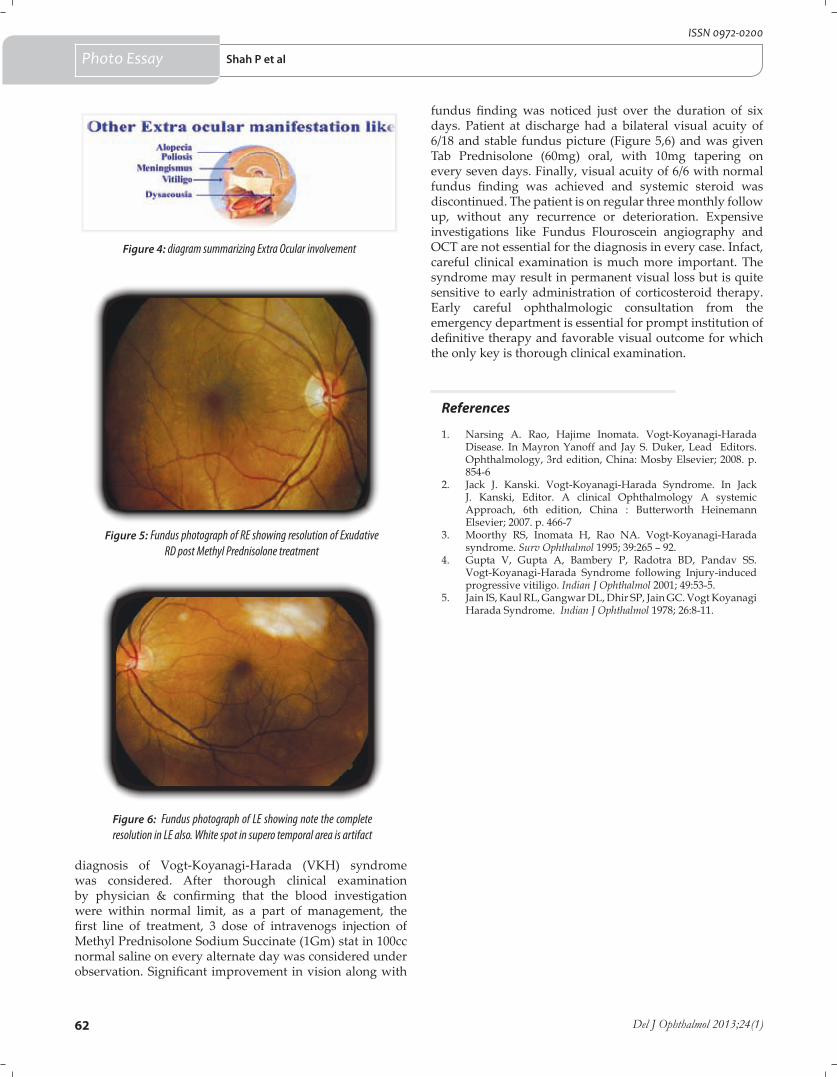
62 Del J Ophthalmol 2013;24(1)
ISSN 0972-0200
References
1. Narsing A. Rao, Hajime Inomata. Vogt-Koyanagi-Harada Disease. In Mayron Yanoff and Jay S. Duker, Lead Editors. Ophthalmology, 3rd edition, China: Mosby Elsevier; 2008. p. 854-6
2. Jack J. Kanski. Vogt-Koyanagi-Harada Syndrome. In Jack J. Kanski, Editor. A clinical Ophthalmology A systemic Approach, 6th edition, China : Butterworth Heinemann Elsevier; 2007. p. 466-7
3. Moorthy RS, Inomata H, Rao NA. Vogt-Koyanagi-Harada syndrome. Surv Ophthalmol 1995; 39:265 – 92.
4. Gupta V, Gupta A, Bambery P, Radotra BD, Pandav SS. Vogt-Koyanagi-Harada Syndrome following Injury-induced progressive vitiligo. Indian J Ophthalmol 2001; 49:53-5.
5. Jain IS, Kaul RL, Gangwar DL, Dhir SP, Jain GC. Vogt Koyanagi Harada Syndrome. Indian J Ophthalmol 1978; 26:8-11.
Photo Essay Shah P et al
diagnosis of Vogt-Koyanagi-Harada (VKH) syndrome was considered. After thorough clinical examination by physician & confirming that the blood investigation were within normal limit, as a part of management, the first line of treatment, 3 dose of intravenogs injection of Methyl Prednisolone Sodium Succinate (1Gm) stat in 100cc normal saline on every alternate day was considered under observation. Significant improvement in vision along with
Figure 4: diagram summarizing Extra Ocular involvement
Figure 5: Fundus photograph of RE showing resolution of Exudative RD post Methyl Prednisolone treatment
Figure 6: Fundus photograph of LE showing note the complete resolution in LE also. White spot in supero temporal area is artifact
fundus finding was noticed just over the duration of six days. Patient at discharge had a bilateral visual acuity of 6/18 and stable fundus picture (Figure 5,6) and was given Tab Prednisolone (60mg) oral, with 10mg tapering on every seven days. Finally, visual acuity of 6/6 with normal fundus finding was achieved and systemic steroid was discontinued. The patient is on regular three monthly follow up, without any recurrence or deterioration. Expensive investigations like Fundus Flouroscein angiography and OCT are not essential for the diagnosis in every case. Infact, careful clinical examination is much more important. The syndrome may result in permanent visual loss but is quite sensitive to early administration of corticosteroid therapy. Early careful ophthalmologic consultation from the emergency department is essential for prompt institution of definitive therapy and favorable visual outcome for which the only key is thorough clinical examination.

63www.djo.org.in
E-ISSN 0976-2892
Brief Communication
Spontaneous Closure of Traumatic Macular Hole
Retina Department, Tejas Eye Hospital, Mandvi, District, Surat, Gujarat*Author for correspondence
Khushboo Doctor DO, FNERF (Retina)
Retina Department, Tejas Eye Hospital, Mandvi, District, Surat, Gujarat, Indiae mail id : [email protected]
Dear Editor, We read with interest the article written by Lalit Verma
et al1 describing “spontaneous resolution of traumatic macular hole” in a 9 year old girl with choroidal rupture with subretinal haemorrhage & vitreous haemorrhage inferiorly in right eye. We would like to congratulate authors for their very nice case report. We would like to make few comments on the case report. Full thickness macular hole was confirmed on spectral domain OCT Scan & there was no vitreous traction on OCT. OCT complements fundus biomicroscopy findings in the evaluation of stage of hole & vitreous adhesion. Moreover, it helps in the detection of subclinical inner retinal layer defect. Patient was kept on observation as child’s parents deferred surgery to a later date due to her academic examination & patient was followed up regularly. Close follow up is required to monitor for development of hole. Visual acuity improved gradually in follow up visits & serial fundus photos & OCT scans showing improvement and at seven months, there was type 2 closure of traumatic macular hole with improvement in visual acuity.
The exact mechanism of Traumatic Macular Hole (TMH) formation remains controversial. It has been suggested that blunt trauma produces a sudden compression and expansion of the globe, which can exert significant stress on the retina, specifically at points of vitreous attachment. Yanagiya et al theorized that the force of impact when transmitted to the macula results in the rupture of the fovea.2 Others hypothesize that the cause may be sudden separation of the posterior vitreous, however many patients present with no posterior vitreous detachment.1-3 Spontaneous closure of
*Khushboo Doctor, Uday Gajiwala, Rohan Chariwala, Kamini Patel
TMH is not so common. Despite the good results obtained by present surgical techniques, we should wait for some time before indicating unnecessary vitreo-retinal surgery in young patient with traumatic macular hole. Spontaneous closure of traumatic macular hole may be much higher in traumatic cases than idiopathic cases. Other factors associated with spontaneous closure of hole are young age, small size of macular hole and absence of posterior vitreous detachment.
We would like to share similar case who presented to us following blunt trauma. A 14 year old boy presented with history of decreased vision in his right eye for 3 days. Patient had loss of visual acuity after ocular impact in right eye with Tennis ball while playing cricket. Vision in right eye was 20/40 & left eye was 20/20. Anterior segment examination was normal. Intraocular pressure (IOP) was normal. Slit lamp biomicroscopy revealed macular hole with Berlin’s Edema of inferonasal foveal predominance. (Figure 1) OCT image showed presence of 285 microm macular hole. (Figure 2) The Amsler Grid showed central alteration & metamorphopsia. Watzke Allen Test was positive. The treatment given was oral prednisolone 1 mg/kg/day in a descending guideline along with gastric protection and Nepafenac (0.1%) Eye drops were given 3 times per day. After 4 weeks, vision had improved to 20/30 in the right eye with Type 1 closure of TMH (Figure 3). OCT confirmed that the macular hole was closed with size 228 microns (Figure 4).
Four mechanisms that have been suggested for spontaneous closure of these holes include; posterior vitreous detachment, release of traction placed on the fovea by the detachment of the posterior hyaloid in the perifoveal area, cell proliferation to fill in the hole, bridging over of retinal tissue and the formation of a contractile epiretinal membrane to close the hole.4-8
Figure1: Color fundus photo of right eye at presentation showing TMH following blunt trauma with Berlin’s Edema of inferonasal predominance
Delhi J Ophthalmol 2013; 24 (1): 63-64
DOI: http://dx.doi.org/10.7869/djo.2013.13
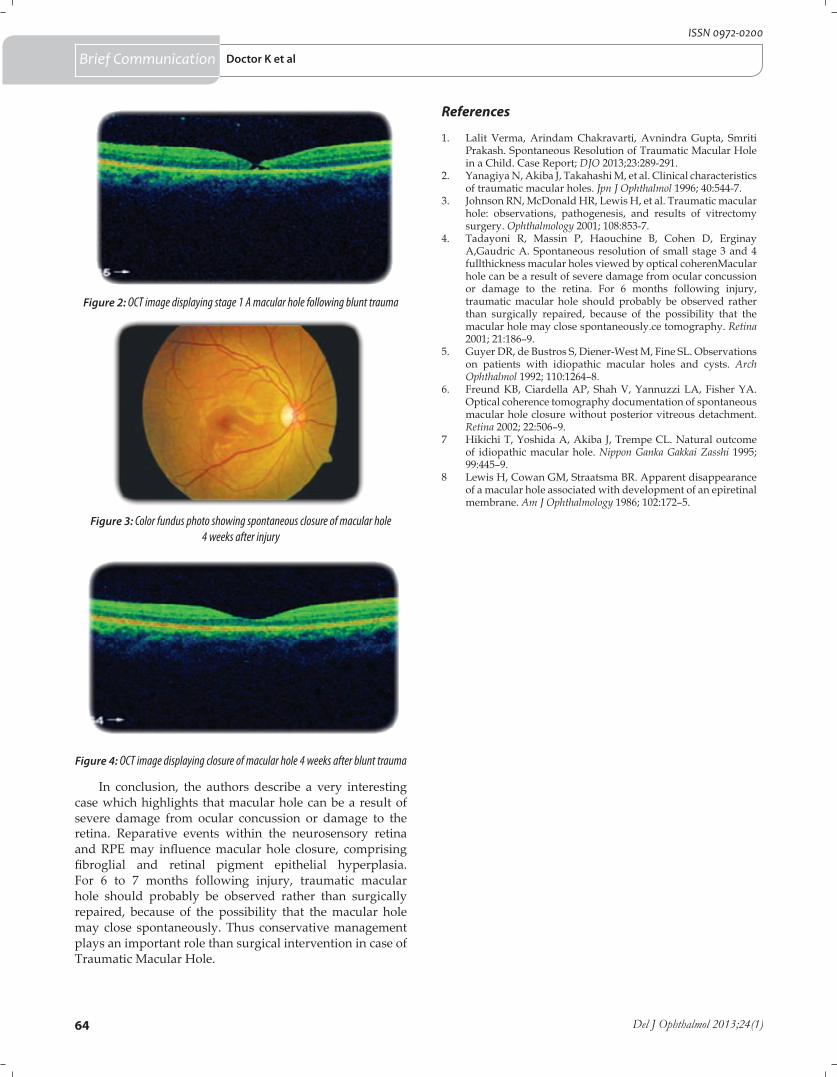
64 Del J Ophthalmol 2013;24(1)
ISSN 0972-0200
Figure 2: OCT image displaying stage 1 A macular hole following blunt trauma
Figure 4: OCT image displaying closure of macular hole 4 weeks after blunt trauma
References
1. Lalit Verma, Arindam Chakravarti, Avnindra Gupta, Smriti Prakash. Spontaneous Resolution of Traumatic Macular Hole in a Child. Case Report; DJO 2013;23:289-291.
2. Yanagiya N, Akiba J, Takahashi M, et al. Clinical characteristics of traumatic macular holes. Jpn J Ophthalmol 1996; 40:544-7.
3. Johnson RN, McDonald HR, Lewis H, et al. Traumatic macular hole: observations, pathogenesis, and results of vitrectomy surgery. Ophthalmology 2001; 108:853-7.
4. Tadayoni R, Massin P, Haouchine B, Cohen D, Erginay A,Gaudric A. Spontaneous resolution of small stage 3 and 4 fullthickness macular holes viewed by optical coherenMacular hole can be a result of severe damage from ocular concussion or damage to the retina. For 6 months following injury, traumatic macular hole should probably be observed rather than surgically repaired, because of the possibility that the macular hole may close spontaneously.ce tomography. Retina 2001; 21:186–9.
5. Guyer DR, de Bustros S, Diener-West M, Fine SL. Observations on patients with idiopathic macular holes and cysts. Arch Ophthalmol 1992; 110:1264–8.
6. Freund KB, Ciardella AP, Shah V, Yannuzzi LA, Fisher YA. Optical coherence tomography documentation of spontaneous macular hole closure without posterior vitreous detachment. Retina 2002; 22:506–9.
7 Hikichi T, Yoshida A, Akiba J, Trempe CL. Natural outcome of idiopathic macular hole. Nippon Ganka Gakkai Zasshi 1995; 99:445–9.
8 Lewis H, Cowan GM, Straatsma BR. Apparent disappearance of a macular hole associated with development of an epiretinal membrane. Am J Ophthalmology 1986; 102:172–5.
Doctor K et al
In conclusion, the authors describe a very interesting case which highlights that macular hole can be a result of severe damage from ocular concussion or damage to the retina. Reparative events within the neurosensory retina and RPE may influence macular hole closure, comprising fibroglial and retinal pigment epithelial hyperplasia. For 6 to 7 months following injury, traumatic macular hole should probably be observed rather than surgically repaired, because of the possibility that the macular hole may close spontaneously. Thus conservative management plays an important role than surgical intervention in case of Traumatic Macular Hole.
Brief Communication
Figure 3: Color fundus photo showing spontaneous closure of macular hole 4 weeks after injury
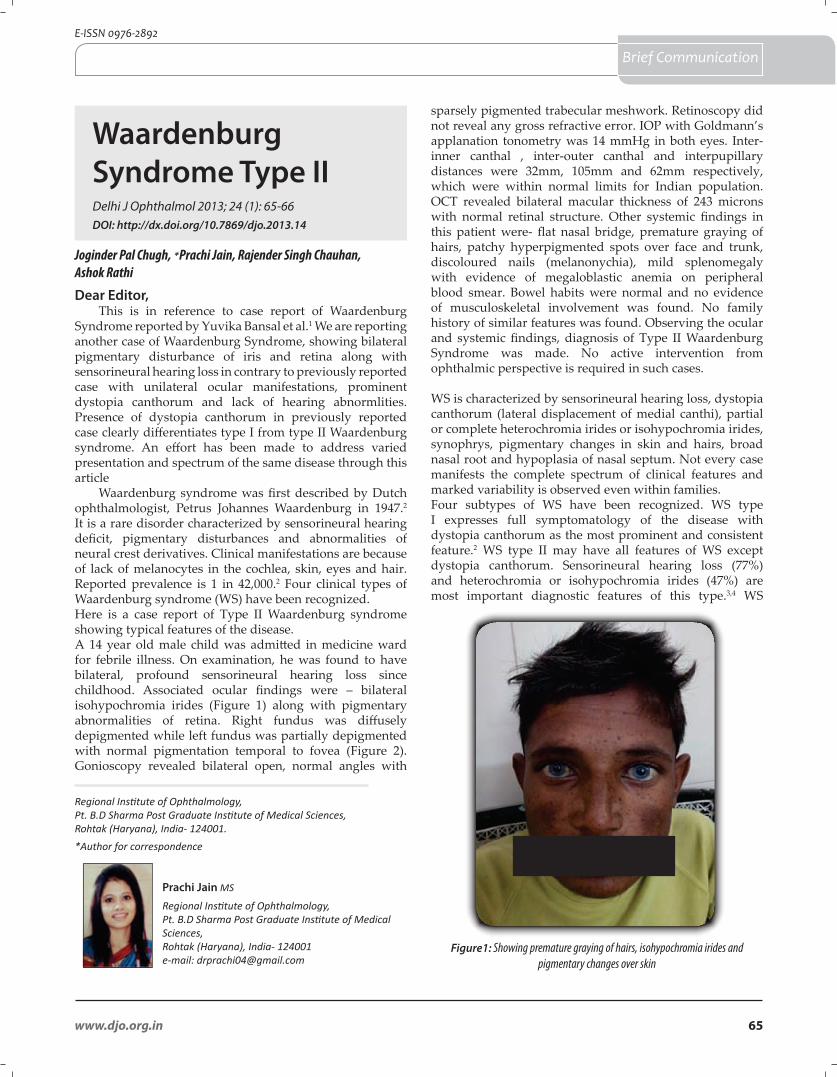
65www.djo.org.in
E-ISSN 0976-2892
Brief Communication
Waardenburg Syndrome Type II
Joginder Pal Chugh, *Prachi Jain, Rajender Singh Chauhan, Ashok Rathi
Dear Editor, This is in reference to case report of Waardenburg
Syndrome reported by Yuvika Bansal et al.1 We are reporting another case of Waardenburg Syndrome, showing bilateral pigmentary disturbance of iris and retina along with sensorineural hearing loss in contrary to previously reported case with unilateral ocular manifestations, prominent dystopia canthorum and lack of hearing abnormlities. Presence of dystopia canthorum in previously reported case clearly differentiates type I from type II Waardenburg syndrome. An effort has been made to address varied presentation and spectrum of the same disease through this article
Waardenburg syndrome was first described by Dutch ophthalmologist, Petrus Johannes Waardenburg in 1947.2 It is a rare disorder characterized by sensorineural hearing deficit, pigmentary disturbances and abnormalities of neural crest derivatives. Clinical manifestations are because of lack of melanocytes in the cochlea, skin, eyes and hair. Reported prevalence is 1 in 42,000.2 Four clinical types of Waardenburg syndrome (WS) have been recognized. Here is a case report of Type II Waardenburg syndrome showing typical features of the disease. A 14 year old male child was admitted in medicine ward for febrile illness. On examination, he was found to have bilateral, profound sensorineural hearing loss since childhood. Associated ocular findings were – bilateral isohypochromia irides (Figure 1) along with pigmentary abnormalities of retina. Right fundus was diffusely depigmented while left fundus was partially depigmented with normal pigmentation temporal to fovea (Figure 2). Gonioscopy revealed bilateral open, normal angles with
Regional Institute of Ophthalmology, Pt. B.D Sharma Post Graduate Institute of Medical Sciences, Rohtak (Haryana), India- 124001.*Author for correspondence
Prachi Jain MS
Regional Institute of Ophthalmology, Pt. B.D Sharma Post Graduate Institute of Medical Sciences, Rohtak (Haryana), India- 124001e-mail: [email protected]
sparsely pigmented trabecular meshwork. Retinoscopy did not reveal any gross refractive error. IOP with Goldmann’s applanation tonometry was 14 mmHg in both eyes. Inter-inner canthal , inter-outer canthal and interpupillary distances were 32mm, 105mm and 62mm respectively, which were within normal limits for Indian population. OCT revealed bilateral macular thickness of 243 microns with normal retinal structure. Other systemic findings in this patient were- flat nasal bridge, premature graying of hairs, patchy hyperpigmented spots over face and trunk, discoloured nails (melanonychia), mild splenomegaly with evidence of megaloblastic anemia on peripheral blood smear. Bowel habits were normal and no evidence of musculoskeletal involvement was found. No family history of similar features was found. Observing the ocular and systemic findings, diagnosis of Type II Waardenburg Syndrome was made. No active intervention from ophthalmic perspective is required in such cases. WS is characterized by sensorineural hearing loss, dystopia canthorum (lateral displacement of medial canthi), partial or complete heterochromia irides or isohypochromia irides, synophrys, pigmentary changes in skin and hairs, broad nasal root and hypoplasia of nasal septum. Not every case manifests the complete spectrum of clinical features and marked variability is observed even within families.Four subtypes of WS have been recognized. WS type I expresses full symptomatology of the disease with dystopia canthorum as the most prominent and consistent feature.2 WS type II may have all features of WS except dystopia canthorum. Sensorineural hearing loss (77%) and heterochromia or isohypochromia irides (47%) are most important diagnostic features of this type.3,4 WS
Figure1: Showing premature graying of hairs, isohypochromia irides and pigmentary changes over skin
Delhi J Ophthalmol 2013; 24 (1): 65-66DOI: http://dx.doi.org/10.7869/djo.2013.14
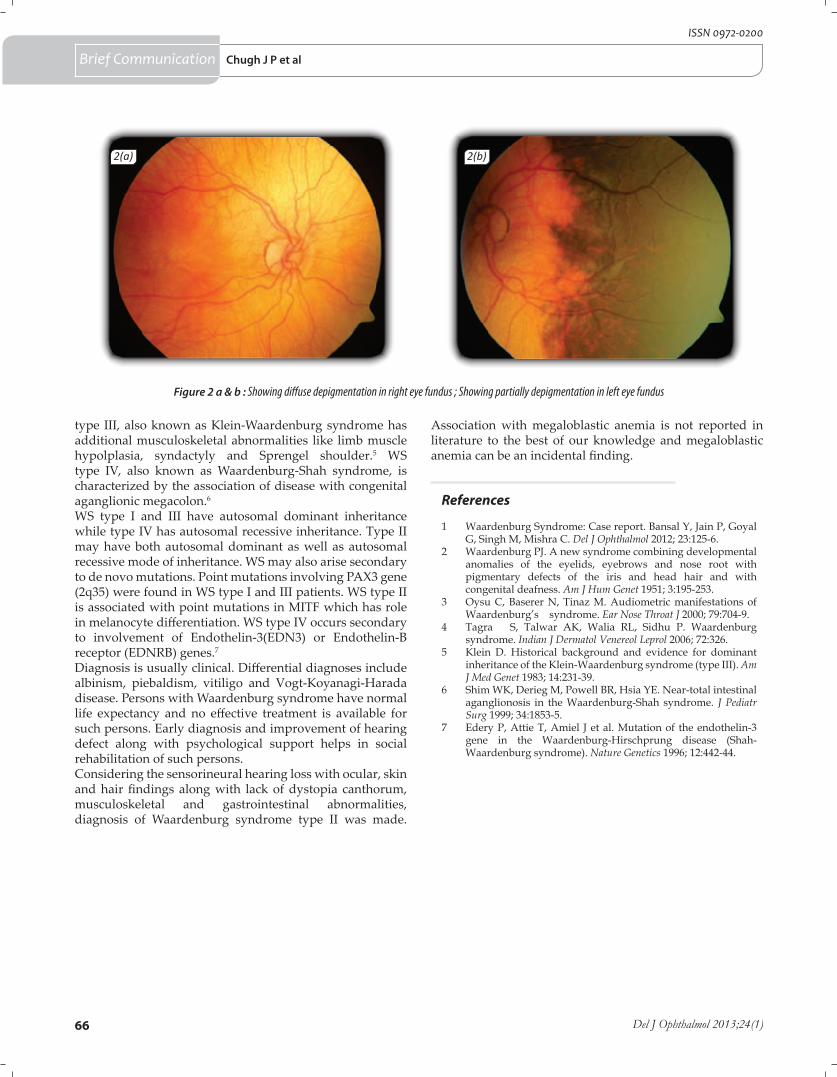
66 Del J Ophthalmol 2013;24(1)
ISSN 0972-0200
type III, also known as Klein-Waardenburg syndrome has additional musculoskeletal abnormalities like limb muscle hypolplasia, syndactyly and Sprengel shoulder.5 WS type IV, also known as Waardenburg-Shah syndrome, is characterized by the association of disease with congenital aganglionic megacolon.6
WS type I and III have autosomal dominant inheritance while type IV has autosomal recessive inheritance. Type II may have both autosomal dominant as well as autosomal recessive mode of inheritance. WS may also arise secondary to de novo mutations. Point mutations involving PAX3 gene (2q35) were found in WS type I and III patients. WS type II is associated with point mutations in MITF which has role in melanocyte differentiation. WS type IV occurs secondary to involvement of Endothelin-3(EDN3) or Endothelin-B receptor (EDNRB) genes.7
Diagnosis is usually clinical. Differential diagnoses include albinism, piebaldism, vitiligo and Vogt-Koyanagi-Harada disease. Persons with Waardenburg syndrome have normal life expectancy and no effective treatment is available for such persons. Early diagnosis and improvement of hearing defect along with psychological support helps in social rehabilitation of such persons.Considering the sensorineural hearing loss with ocular, skin and hair findings along with lack of dystopia canthorum, musculoskeletal and gastrointestinal abnormalities, diagnosis of Waardenburg syndrome type II was made.
Figure 2 a & b : Showing diffuse depigmentation in right eye fundus ; Showing partially depigmentation in left eye fundus
2(a) 2(b)
Association with megaloblastic anemia is not reported in literature to the best of our knowledge and megaloblastic anemia can be an incidental finding.
References
1 Waardenburg Syndrome: Case report. Bansal Y, Jain P, Goyal G, Singh M, Mishra C. Del J Ophthalmol 2012; 23:125-6.
2 Waardenburg PJ. A new syndrome combining developmental anomalies of the eyelids, eyebrows and nose root with pigmentary defects of the iris and head hair and with congenital deafness. Am J Hum Genet 1951; 3:195-253.
3 Oysu C, Baserer N, Tinaz M. Audiometric manifestations of Waardenburg’s syndrome. Ear Nose Throat J 2000; 79:704-9.
4 Tagra S, Talwar AK, Walia RL, Sidhu P. Waardenburg syndrome. Indian J Dermatol Venereol Leprol 2006; 72:326.
5 Klein D. Historical background and evidence for dominant inheritance of the Klein-Waardenburg syndrome (type III). Am J Med Genet 1983; 14:231-39.
6 Shim WK, Derieg M, Powell BR, Hsia YE. Near-total intestinal aganglionosis in the Waardenburg-Shah syndrome. J Pediatr Surg 1999; 34:1853-5.
7 Edery P, Attie T, Amiel J et al. Mutation of the endothelin-3 gene in the Waardenburg-Hirschprung disease (Shah-Waardenburg syndrome). Nature Genetics 1996; 12:442-44.
Chugh J P et alBrief Communication
67www.djo.org.in
E-ISSN 0976-2892
Letter to editor
Echographic Evaluation of Retinoblastoma and Its Management Modalities
Dear EditorThis letter is about the article Echographic Evaluation of
retinoblastoma and its management modalities, published in DJO 2013; 23 (4).1 We agree with the authors that in the Indian context, presentation of retinoblastoma in the advanced stage of the disease is more common compared to Western literature mainly because of the lack of awareness and delayed diagnosis. Ultrasound B scan is an extremely sensitive and inexpensive modality for the diagnosis of intraocular retinoblastoma and should be done in all children suspected of having retinoblastoma. However, role of B scan is limited to diagnosis of mainly intraocular tumors and role of other imaging modalities should not be underemphasized. In patients with extraocular extension of the disease, other imaging modalities like CT scan or MRI is a must to note the extraocular extent of the disease and possible intracranial extension. Gross proptosis or a fungating extraocular mass clearly indicates an extraocular extension of the disease. However, early cases of optic nerve invasion can manifest only with a subtle prominence of the globe in an eye with apparent intraocular disease. Hence, globe prominence should be looked for in all cases of retinoblastoma and if present a MRI or CT scan is a must in those cases before deciding on the treatment.
About the management outcome, it would have been better if the authors had provided data about stage of presentation and the management outcome of all 100 patients. In authors series, 18 eyes were enucleated 2 of which showed regrowth, possibly orbital recurrence. Authors have not provided information about the presence or absence of histopathological high risk factors on these 18 eyes and whether the optic nerve transaction was involved by tumor cells in these 2 cases which showed a local recurrence. As per the current management protocol, histopathological evaluation of the enucleated eyeball by an ocular oncopathologist is a must to look for certain high risk factors. Only patients having high risk factors should receive adjuvant chemotherapy which can decrease the risk of metastasis from 24% to 4%.2 Authors have also
Sima Das MS Oculoplasty and Ocular Oncology Services
Dr Shroff’s Charity Eye HospitalDaryaganj, New Delhi
e-mail: [email protected]
not mentioned if the cases with local recurrence had only intraocular tumor to begin with or had involvement of the optic nerve on preoperative CT or MRI. Cases with involvement of the optic nerve or extraocular extension preoperatively should receive neoadjuvant chemotherapy before taking up for enucleation or exenteration to reduce the risk of recurrence and metastasis.
Authors conclude that the response of chemotherapy and laser for treatment of retinoblastoma is promising but not predictable. Authors have provided data on treatment response of 20 patients who have received combined therapy. However, the stage and group of the disease is not mentioned for those patients. Response to combined (chemotherapy and /or adjuvant therapy like laser, cryotherapy, transpupillary thermotherapy, brachytherapy for intraocular retinoblastoma depends on the grouping of the tumor with 100% tumor control reported in Group A eyes and 47% in Group D eyes.3 The current management strategy for intraocular retinoblastoma includes chemoreduction with or without focal therapy as the primary management modality and radiotherapy and enucleation being used for more advanced cases. The current management protocol has been reported to provide more than 90% cure rate in the Western setup.4,5
References
1. Delhiwala K S, Thakkar H H. Echographic evaluation of retinoblastoma and its management modalities. Delhi Journal of Ophthal 2013; 23:257–62.
2. Honavar SG, Singh AD, Shields CL, Meadows AT, Demirci H, Cater J, Shields JA Postenucleation adjuvant therapy in high-risk retinoblastoma. Arch Ophthalmol 2002; 120:923-31.
3. Shields CL, Mashayekhi A, Au AK, Czyz C, Leahey A, Meadows AT, Shields JA. The International Classification of Retinoblastoma predicts chemoreduction success.Ophthalmology 2006; 113:2276-80. Epub 2006 Sep 25.
4. Shields CL, Shields JA, Needle M, de Potter P, Kheterpal S, Hamada A, Meadows AT. Combined chemoreduction and adjuvant treatment for intraocular retinoblastoma Ophthalmology 1997; 104:2101-11.
5. Shields CL, Shields JA. Recent developments in the management of retinoblastoma. J Pediatr Ophthalmol Strabismus 1999; 36:8-18.
Delhi J Ophthalmol 2013; 24 (1): 67DOI: http://dx.doi.org/10.7869/djo.2013.15
68 Del J Ophthalmol 2013;24(1)
ISSN 0972-0200
Letter to editor
Comparison of Ultrasound Biomicroscopy and Gonioscopy Features of Angle In Pre & Post Laser Peripheral Iridotomy Patients of Primary Angle Closure Glaucoma
Dear EditorWe have read the article “Comparison of Ultrasound
Biomicroscopy and Gonioscopy Features of Angle In Pre & Post Laser Peripheral Iridotomy Patients of Primary Angle Closure Glaucoma” in DJO April – Jun 2013 by Prajapati et al.1 It was an interesting article but we would like to raise following points for discussion:1. The authors have included newly diagnosed patients of
Acute and Chronic PACG of > 20 years of age. Why the cut off for the age was taken as 20 years, is not clearly mentioned. This is not the usual age described for primary glaucomas.
2. The Acute PACG group had 20 eyes of 12 patients. It seems that 8 eyes had bilateral acute attack at presentation. Acute PACG is usually unilateral to present. Whether other secondary possible causes for acute attack were investigated or history for any drug intake was elucidated?
3. The timing for peripheral iridotomy (PI) in the eyes with Acute PACG is also not clear. Moreover, was it possible to do primary PI in all the patients of Acute PACG? If not, then what else was done in these patients and whether those patients were included in the study?
4. The authors have also not clarified that while doing UBM whether the patient was asked to fixate at a predetermined target, because this can also affect the angle parameters.
5. The result section mentions that the criterion for diagnosing Acute and chronic PACG are mentioned
earlier. But they could not be found in material or methods. The extent of PAS taken up in the diagnosis of PACG and the extent to which they really opened up after peripheral iridotomy in the eyes with chronic PACG is not very clear.
6. The result section mentions that after 1 weeks of YAG PI, no angles were closed. That means all angles open up after laser PI that might not be true in the cases of chronic PACG. The discussion also mentions that Dada et al found that angles don’t open in chronic PACG due to synechia looks more logical.2 The appositional angles can surely open up after YAG PI. A recent study has also highlighted that quadrants unaffected by PAS can be expected to widen as much as in eyes with only appositional closure. In quadrants with PAS the ultrasound biomicroscopy parameters did not change following laser PI.3
7. The material and methods section mentions that the gonioscopic findings were recorded only in the temporal quadrant, and discussion says that the UBM parameters were assessed in all the four quadrant? So, why the mean of 4 quadrants of UBM parameters was compared to only temporal gonioscopic values?
8. The authors concluded in their last point that the early diagnosis of angle closure is possible by UBM. But subtle signs of angle closure like iris atrophy, entropion uvea, patchy pigmentation of angles etc. cannot be seen by UBM that are easily seen by slit lamp and goniscope.4
Shalini Mohan MS, DNB, MNAMS Assistant ProfessorGlaucoma Services,
Department of OphthalmologyGSVM Medical College, Kanpur
Email: [email protected]
References
1. Vaishali AP, Viral R, Mariam NM, Purvi B, Prajapati K, Nirav M. Comparison of Ultrasound Biomicroscopic and Gonioscopic Features of Angle In Pre & Post Laser Peripheral Iridotomy Patients of Primary Angle Closure Glaucoma. Del J Ophthalmol 2012; 23:263-6.
2. Dada T, Mohan S, Sihota R, et al. Comparison of ultrasound biomicroscopic parameters after laser iridotomy in eyes with primary angle closure and primary angle closure glaucoma. Eye (Lond) 2007; 21:956-61.
3. Lin Z, Liang Y, Wang N, Li S, Mou D, Fan S, Sun S, Tang X, Thomas R. Peripheral Anterior Synechia Reduce Extent of Angle Widening After Laser Peripheral Iridotomy in Eyes With Primary Angle Closure. J Glaucoma 2013; 22:374-9.
4. Sihota R, Saxena R, Agarwal HC. Entropion uveae: early sphincter atrophy, sign posting primary angle closure glaucoma? Eur J Ophthalmol 2004; 14:290-7.
*Shalini Mohan, Ramesh Chandra Gupta, Perwez Khan, Rajnath Singh Kushwaha, Surendra Kumar Sachan
Delhi J Ophthalmol 2013; 24 (1): 68-69DOI: http://dx.doi.org/10.7869/djo.2013.16

69www.djo.org.in
E-ISSN 0976-2892
Author’s reply
Dear EditorWe thank Drs S Mohan et al for their interest in our
article on Comparison of Ultrasound Biomicroscopy and Gonioscopy Features of Angle in Pre & Post Laser Peripheral Iridotomy Patients of Primary Angle Closure Glaucoma.1 Our responses to their queries are as follows: 1. In our study, we had taken 20years demographic data.2. We agree that acute PACG is almost always unilateral,
but our centre being a tertiary referral institute, we get cases with bilateral presentations. A detailed history was taken in all cases to rule out secondary causes and any factor which might have possibly lead to bilateral acute angle closure, including drug intake.
3. The peripheral iriditomy was done on same day in all cases. Before peripheral iriditomy, medical management was instituted if needed, in form of Injection mannitol, oral acetazolamide, topical timolol and pilocarpine to lower the IOP and to clear the cornea to enable us to perform a peripheral iriditomy.
4. While doing UBM, the patients were asked to fixate at a distant target to eliminate any effect of accommodation.
5. The criterion for inclusion and exclusion in the study has been mentioned. We have diagnosed acute and chronic PACG according to the standard criteria and guidelines. The extent of peripheral anterior synechiae (PAS) and their opening has been not mentioned as it has not been a part of our study. Our aim was to study angle parameters on UBM and establish its usefulness. Out of 20 eyes that presented with acute PACG, 12 (60%) had completely closed angle (grade 0), while 8 (40%) of them had grade 1. Post laser peripheral iridectomy (LPI), 2 (10) out of 20 eyes remained closed angle; 9 (45%) eyes had grade 1, while 9 (45%) eyes improved to grade 2. Among grade I post LPI, 2 eyes remained grade I as of pre LPI.
6. Out of 50 eyes of chronic PACG, 10 (20%), 19 (38%) & 21 (42%) eyes had grades 0, 1, 2 respectively. Post LPI, there was no eye with completely closed angle and 8 (16%), 31 (62%), 11 (22%) eyes had grade 1, 2 & 3 respectively. Out of Grade I Post LPI, 2 eyes had same Grade I angle grading as of Pre LPI & 7 eyes had no improvement in Pre LPI Grade II angle, and remained in Grade II Post LPI. The results indicate that all angles have not opened up.
7. Gonioscopy was performed in all quadrants but only temporal quadrant/angle was used for the sake of uniformity. Similarly, UBM measurements were considered only in the temporal quadrant of all eyes for sake of uniformity and most of the studies done with UBM have used temporal angles for their study.2-4
8. We do not underestimate the importance of clinical assessment and gonioscopy. Till date, they are the basis and gold standard ways for diagnosing glaucoma. But our aim in this study was to establish the usefulness of UBM as an additional tool in glaucoma diagnosis and management. Patients with acute rise of IOP, often
present with corneal oedema which prevents conclusive gonioscopy. These are the cases where UBM has an upper edge. An additional advantage of UBM is that it provides objective evaluation, allows for measurements and has the scope for documentation.
Vaishali AP MSM & J Western Regional Institute of Ophthalmology
Civil hospital, AhmedabadGujarat - 380013, India
e-mail - [email protected]
*Vaishali AP, Viral R, Mariam NM, Purvi B, Prajapati K, Nirav M
References
1. Vaishali AP, Viral R, Mariam NM, Purvi B, Prajapati K, Nirav M. Comparison of Ultrasound Biomicroscopic and Gonioscopic Features of Angle In Pre & Post Laser Peripheral Iridotomy Patients of Primary Angle Closure Glaucoma. Del J Ophthalmol 2012; 23:263-66.
2. Sushmita Kaushik, Rajeev Jain, Surinder Singh Pandav, Amod Gupta. Evaluation of the anterior chamber angle in Asian Indian eyes by ultrasound biomicroscopy and gonioscopy. Indian Journal of Ophthalmology 2006; 54:159-63.
3. Dada T, Mohan S, Sihota R, et al. Comparison of ultrasound biomicroscopic parameters after laser iridotomy in eyes with primary angle closure and primary angle closure glaucoma. Eye (Lond) 2007; 21:956-61.
4. Kaushik S, Kumar S, Jain R, Bansal R, Pandav SS, Gupta A. Ultrasound biomicroscopic quantification of the change in anterior chamber angle following laser peripheral iridotomy in early chronic primary angle closure glaucoma. Eye (Lond) 2007; 21:735 - 41. Epub 2006 Mar 17.
Letter to editorAuthor’s reply

70 Del J Ophthalmol 2013;24(1)
ISSN 0972-0200
We accept solicited and unsolicited manuscripts that are not under consideration for publication in any other journal. All submitted manuscriptsaresubjecttoreviewbyindependentexpertsinthefieldthroughanonlinereviewersystem.Youmaysubmityourmanuscriptsalong with a covering letter to Dr M.VANATHI, Editor-in-chief, Delhi Journal of Ophthalmology.
Manuscript SubmissionAll manuscripts are required to be submitted through the online submission portal through the journal website: www.djo.org.in.incaseofanyqueriespleasecontacttheeditorialofficeattheafteraddresseditordjo2013@gmail.com
Editorial PolicyDelhi Journal of Ophthalmology titles conform to the Uniform Requirements for Manuscripts Submitted to Biomedical Journals, issued by theInternationalCommitteeforMedicalJournalEditors(October2004).Manuscript submission & processingDelhi Journal of Ophthalmology publishes solicited and unsolicited articles. Acknowledgement of receipt of all manuscripts will be sent to the corresponding author, once the editorial desk reviews the manuscript for conforming to the requirements of the journal. The initial screeningofthearticlesbythe internaleditorialstaffassessestheformatting,topicalityand importanceofthesubject, theclarityofpresentation, and relevance to the target audience of the journal.If you are interested in submitting an article, or have any queries regarding article submission, please contact the Editor-in-chief (see Contactdetails).We also have an active commissioning program whereby, under guidance from the Editorial Committee, we solicit articles directly for publication.External reviewInordertoensurethatmanuscriptacceptanceisunbiased,scientificallyaccurateandclinicallyrelevant,allarticlesarereviewedbytwoormoremembersoftheEditorialCommitteeandtheEditorialBoardand/orotherspecialistsintherelatedfields.Reviewisperformedonadouble-blindbasiswhereintheidentitiesofreviewersandauthorsarekeptconfidential.Reviewersmustdisclosepotentialconflictsofintereststhatmayaffecttheirabilitytoprovideanunbiasedappraisal(seeConflictofInterestPolicybelow).RevisionMost manuscripts require some degree of revision prior to acceptance. Corresponding authors are requested to submit the revised manuscript along with one highlighted copy with revisions highlighted. Detailed responses to reviewers’ comments, in a covering letter/email,arealsorequired.ThefinaldecisiononacceptanceofthemanuscriptforpublicationlieswiththeEditor-in-chief.
CopyrightThe corresponding author of the manuscript is responsible for obtaining permissions at the time of submission, to use material presented in the manuscript. Please send us a copy of letters or forms granting you permission for the use of copyrighted material in order to facilitate any special requirements with regard to wording and placement of credits that may be required. The corresponding author will be required to submit a signed copyright transfer form, signed by all co-authors, along with the manuscript at the time of submission, failing which the manuscript will not be considered for review.COPYRIGHT FORM IS AVAILABLE ONLINE
Author disclosure, copyright transfer & conflict of interest policyAuthors are responsible for the content of material and views expressed in the manuscripts. Authors must disclose explicitly conflictsofinterest,financialdisclosures(orthelackofit)thatmayberelevanttothemanuscriptunderconsideration.Thisshouldfigureattheendofthemanuscript,beforethe“References”section.Detailsofrelevantconflictsofinterests(orthelackof)mustbedeclaredinthe‘Disclosure’sectionofthemanuscriptforalllistedauthors. Any such potential conflict of interest (including sources of funding) should be summarized in a separate section of the published article. Externalreviewersmustdiscloseanyconflictsofinterestthatcouldbiastheiropinionsofthemanuscript,andtheyshoulddisqualifythemselvesfromreviewingspecificmanuscriptsiftheybelieveitappropriate.Shouldanysuchconflictofinterestbedeclared,thejournal Editor-in-chief will judge whether the reviewer’s comments should be recognized or will interpret the reviewer’s comments in the context of any such declaration.
Policies on ethical conduct of researchWhere manuscripts include publication of original data relating to human or animal experimental investigations, appropriate institutional review board approval is required and should be described within the article. For those investigators who do not have formal ethics review committees, the principles outlined in the Declaration of Helsinki should be followed. For investigations involving human subjects, authors should explain how informed consent was obtained from the participants involved. Identifying information should not be included unless theinformationisessentialforscientificpurposesandwritteninformedconsentistakenforpublication.Inattemptingtomaintainpatientanonymity,identifyingdetailsshouldbeomittedwheretheyarenotessential.However,patientdatashouldneverbeamendedorfalsified.
Author Guidelines
Our complete Author Guidelines is available at www.djo.org.in
71www.djo.org.in
E-ISSN 0976-2892
Informed consent should be obtained whenever there is any doubt that anonymity can be assured.
Manuscript PreparationDetails for manuscript preparation include:Manuscripts of the following types may be submitted:
Major Review : Manuscriptssubmittedinthissectionshouldbewithin3000wordslimit,withanunstructuredabstractof400words
Recent Advances: Manuscriptssubmittedinthissectionshouldbewithin3000wordlimitwithanunstructuredabstractof400words
Original Article: Manuscriptssubmittedinthissectionshouldbewithin3000wordlimit(text)withastructuredabstractof400words
YOUNG OPHTHALMOLOGIST CORNER: Postgraduates are urged to submit their thesis work, in the current year of completion of their , as original article, to this section. A certificate to this effect signed by all the co-authors and the head of institution to which the postgraduate belongs is to be submitted along with the manuscript. This may also be stated in the accompanying covering letter. Postgraduate thesis work accepted as original article publication in this section will also be eligible to contest for the best paper award.
Techniques: Videos of techniques in ophthalmology, videonotlongerthan8minutesinMPEG2formatwithtitle,credentialsofpresentingauthors,disclosures,conflictof interest,acknowledgementsandanyother relevantdetails is tobe included.Theophthalmicsurgicaltechnique is to be explicitly detailed in clear English narration. All relevant steps of surgery are to be lucidly described and depicted in thevideo.Thevideoshouldbeaccompaniedwithmanuscriptof1000words(unstructuredabstract,keywords,textwithsubheadingofintroduction,principle,surgicaltechnique,disclosures)andreferences.Visualsofhospitalsofthecorrespondingauthorsetcaretobeavoided in the video.
Submissions relating to ophthalmic surgical techniques that would be an apt guidance / instruction material for ophthalmology residents will be preferred. Copyright transfer is mandatory along with the submission. Only solicited submissions will be entertained in this section. Those who wish to submit video techniques may correspond to the EDITOR-IN-CHIEF regarding the same.
Case Reports: Interestingcaseswithimmenseclinicalsignificance/rarecasereportswillbeacceptedinthiscategory.Submissionsinthiscategoryshouldincludeastructuredabstract(300words)withtotaltextwordlimitis1500words
Allied Ophthalmic Sciences: Manuscriptssubmittedinthissectionshouldbewithin3000wordlimitwithanunstructuredabstractof400words. Submissions pertaining to ocular pathology, ocular microbiology, ocular biochemistry, ocular pharmacology, ocular community medicine, ophthalmic hospital administration, optometry & contact lenses will be entertained.
Photo Essay: Submissions in this category should include high quality ophthalmic photography pertaining to an interesting rare case scenariooracaseof teachingsignificancetoophthalmicpostgraduateresidents.Anunstructuredabstractof300word limit is tobeincluded.Themanuscriptshouldbewithin1000words.Allfigurelegendsshouldbeclearanddescriptive.
Brief Communications: Manuscripts in this category includes letters to editors on manuscripts published in the preceding two to three issuesoranysubjectofrelevancetoophthalmologypractices.Thewordlimitforthissectionis500wordsandonlyfivereferences.
Expert’s Deliberations: Each issue will feature a compiled editorial in this section dealing with common ophthalmic clinical case scenarios
All manuscript are required to include the following details: • Titleofthemanuscript• Typeofmanuscript• Forename(s)andsurnamesofauthors(seeAuthorshipsectionbelow)• Authoraffiliations:Department,Institution,andcontactdetails(mailingaddress,emailandcontactmobilenumber)ofallauthors• 3–6keywords,Runningtitle,Noofwordsofabstractandtext(excludingreferences)• Correspondingauthor:name,designationandcredentials,address,phone,fax,emailanddigitalpassportsizephotograph
Formatting Requirements: © Themanuscriptistobesubmittedastwofiles:
(i) FIRST PAGE FILE: This should contain the covering letter, title page with details of all the authors & their affiliations, title of manuscript, acknowledgement and signed authorship form. Please submit as word / pdf files. Do not zip the files.(ii) ARTICLE FILE: This should contain the title, abstract, word counts of abstract & text, text, references, and legends. Figures and tables to be submitted separately. No details regarding identity of authors should be included in this file. Double-spacing of the entire text.
Author Guidelines
72 Del J Ophthalmol 2013;24(1)
ISSN 0972-0200
© Pagenumberingtobedone.Clearconciselanguage,Americanspelling,Tablesandfigurestobequotedintextinorderof appearance and the preferred electronic format for text is Microsoft Word. Generic drug names are to be used in text, tables, andfigures.Suppliersofdrugs,equipment,andotherbrand-namematerialaretobecreditedinparentheses(company,name, city,state,country)© Pleasespelloutacronymsinthefirstinstanceofappearanceintheabstractandpaper© FiguresandTablesaretobesubmittedasseparatefiles.Theyaretobenumberedinthesequenceofappearanceinthetext, with a descriptive heading/legend provided for each. Abbreviations and footnotes are to be placed immediately below the table.FiguresaretobesubmittedasPDFs,TIFFfiles,orintheiroriginatinggraphicsapplication.© Graphics/ contents downloaded from web pages are NOT ACCEPTABLE.© References should be written in standard international format as follows: Authors, title of citation quoted, name of journal, year of publication; volume number: page numbers. © THE CORRESPONDING AUTHOR WILL BE RESPONSIBLE FOR ANY CONCERNS ARISING OUT OF TO PLAGIARISM, AUTHORSHIP OR RELATED ISSUES. © THE JOURNAL OR THE SOCIETY WILL NOT BE RESPONSIBLE FOR THE VIEWS PROJECTED IN THE MANUSCRIPTS. © Authorsmustdiscloseexplicitlyconflictsofinterest,financialdisclosures(orthelackofit),acknowledgements,thatmaybe relevanttothemanuscriptunderconsideration.Thisshouldfigureattheendofthemanuscript,beforethe“References”section.
Please note: MANUSCRIPTS WILL NOT BE ACCEPTED FOR REVIEW IF THESE INSTRUCTIONS ARE NOT FOLLOWED
Please note the Criteria for authorship credit:1)Substantialcontributionstoconceptionanddesign,acquisitionofdata,oranalysisandinterpretationofdata;2)Draftingthearticleorrevisingitcriticallyforimportantintellectualcontent;and3)Finalapprovaloftheversiontobepublished. All contributors who do not meet the criteria for authorship (such as those who provided purely technical help, writing assistance, or a department chairperson who provided only general support) may be listed in the acknowledgments section.
Compliance with Ethical RequirementsConflict of Interest: TheConflictof Intereststatementshould listeachauthorseparatelywithregardstoconflictof interest, researchgrants,speakerhonorarium,financialinterestsetc.Incaseofmultipleauthorsdeclarenoconflict,thismaybestatedseparatelyforeachauthorattheendofthemanuscripttext(beforethereferences).For studies conducted with human subjects, statements pertaining to ethical standards should be included: All procedures followed were inaccordancewiththeethicalstandardsoftheresponsiblecommitteeonhumanexperimentation(institutionalandnational)andwiththeHelsinkiDeclarationof1975,asrevisedin2008.Informedconsentwasobtainedfromallpatientsforbeingincludedinthestudy.Intheevent of lack of clarity if the research was conducted in accordance with the Helsinki Declaration, the authors must explain the rationale for their approach, and demonstrate that the institutional review body explicitly approved the doubtful aspects of the study.If any identifying information about patients is included in the article, the following sentence should also be included: Additional informed consent was obtained from all patients for which identifying information is included in this article.For studies involving animal experiments statements pertaining to ethics standards should be included: All institutional and national guidelines for the care and use of laboratory animals were followed.
Author Guidelines
Contact Details: Dr M.Vanathi MDEditor–in–Chief Delhi Journal of OphthalmologyDOS SecretariatRoom No 479, 4th floorDr R P Centre For Ophthalmic SciencesAIIMS, New Delhi 110029Ph: 65705229, 26588074Email: [email protected]/[email protected]: www.djo.org.in
Advertisement Directory: • AMO (i) Biomedix (ii) • Alcon(iii)•Appasamy(iv)•Biomedix(v)•ChoithramNetralaya(vi)Alcon(vii) •
73www.djo.org.in
E-ISSN 0976-2892
Copyright Form