dr ziad
TRANSCRIPT
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 1/99
CLINICAL AND LABORATORY PROCEDURES INCONSTRUCTION OF
COMPLETE DENTURES
Dr Ziad AL-Dwairi BDS, PhD(UK), FIADFEAssociate Professor of Prosthodontics
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 2/99
Complete Denture
A dental prosthesis that replaces all of
the natural dentition and associated
structures of maxilla and mandible. It
may be supported by mucosa or
sometimes by dental implants.
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 3/99
Esthetic.
Improve mastication.
Improve speech.
Function withoutinterferences.
Preservation of oralstructures.
Maintenance of health &
comfort.
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 4/99
Clinical examination
Tray selection
Primary impression
Primary cast
Secondary impression Secondary cast
Denture base fabrication and Occlusal
rim

7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 5/99
Setting of teeth
Flasking ,dewaxing
And curing
Trimming and polishing
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 6/99
HISTORY ANDEXAMINATION FOR
EDENTULOUS PATIENTS
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 7/99
Objectives
Recognition of relevant anatomical,
physiological and psychologicalconditions
Understand significance of medical
status Development of treatment plan
(prescription of prosthesis)
Assessment of existing dentures
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 8/99
Extra-oral
examination The extra-oral examination should look for :
– Temporo mandibular joint( TMJ):palpate externally and from inside the
ear: pain, clicking, limitation of movement, extreme deviation
– The patients face height,
– Any facial asymmetry including – The centre line;
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 9/99
Extra-oral examination
– The lip line including the smile line as allthese features will need to be transferred
to the patients dentures. –
– The degree of overclosure will also needto be assessed and this will help withdeciding on how you want to make thedenture
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 10/99
Extra-oral examination
– The lip line including the smile line as allthese features will need to be transferred
to the patients dentures. –
– The degree of overclosure will also needto be assessed and this will help withdeciding on how you want to make thedenture
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 11/99
Intra-oral Examination
Soft tissue
Salivary flow
Sulcus depth Ridge anatomy: height, depth and form
(firm or flabby)
Inter-ridge relationships If already wearing dentures: denture
assessment – fit, retention, stability andocclusion. Can you copy this if it is
already satisfactory?
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 12/99
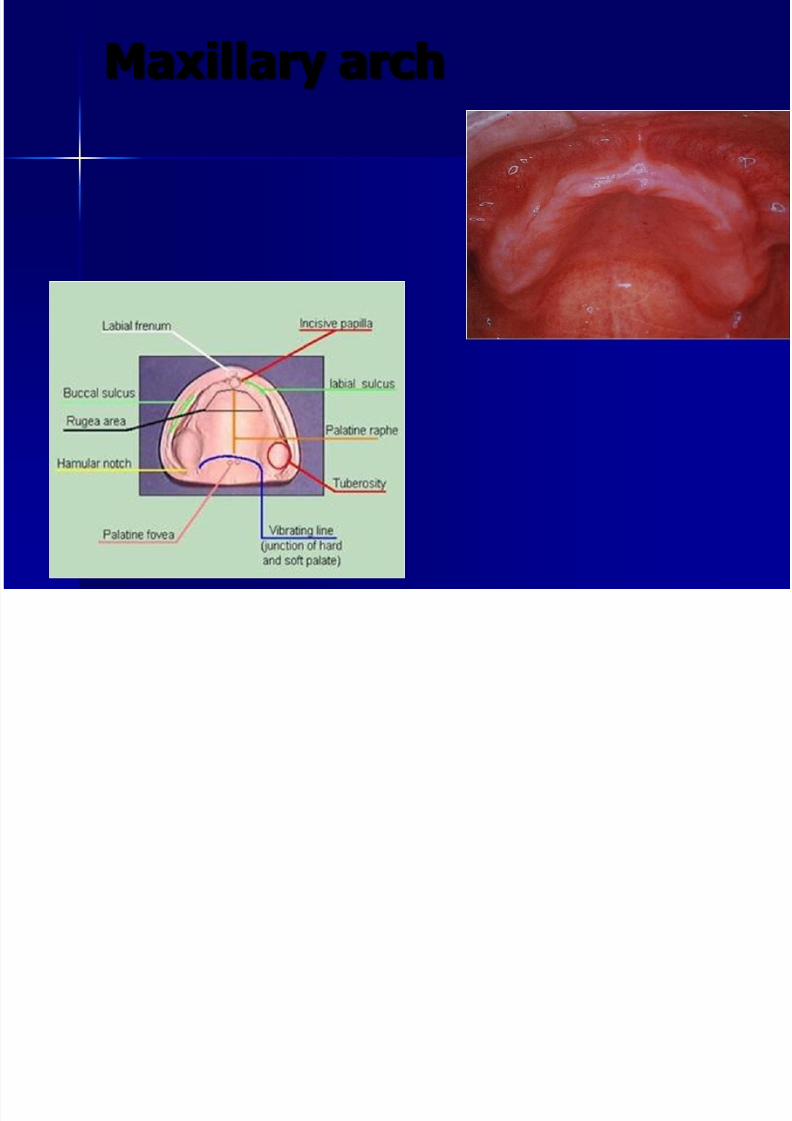
Maxillary arch
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 13/99
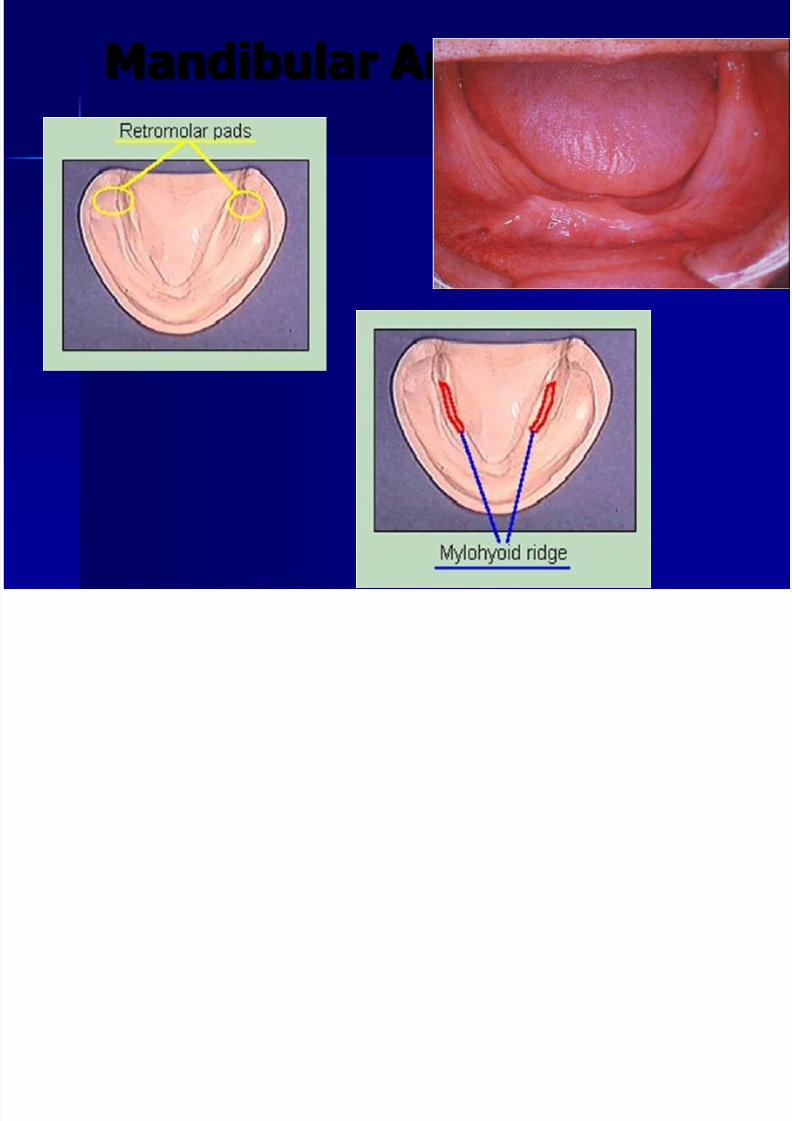
Mandibular Arch
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 14/99
IMPRESSIONS FOR
COMPLETE DENTURES
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 15/99
IMPRESSIONS
Definition: A negative likeness of thetissues so that a model can be madefrom which a denture can be
constructed. The impression material is held against
the tissues and is supported by animpression tray. The material shows
plastic flow in the initial stages and thenhardens.
A model is then formed using modelstone or plaster. For maximum accuracy
a 2 stage impression procedure is

7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 16/99
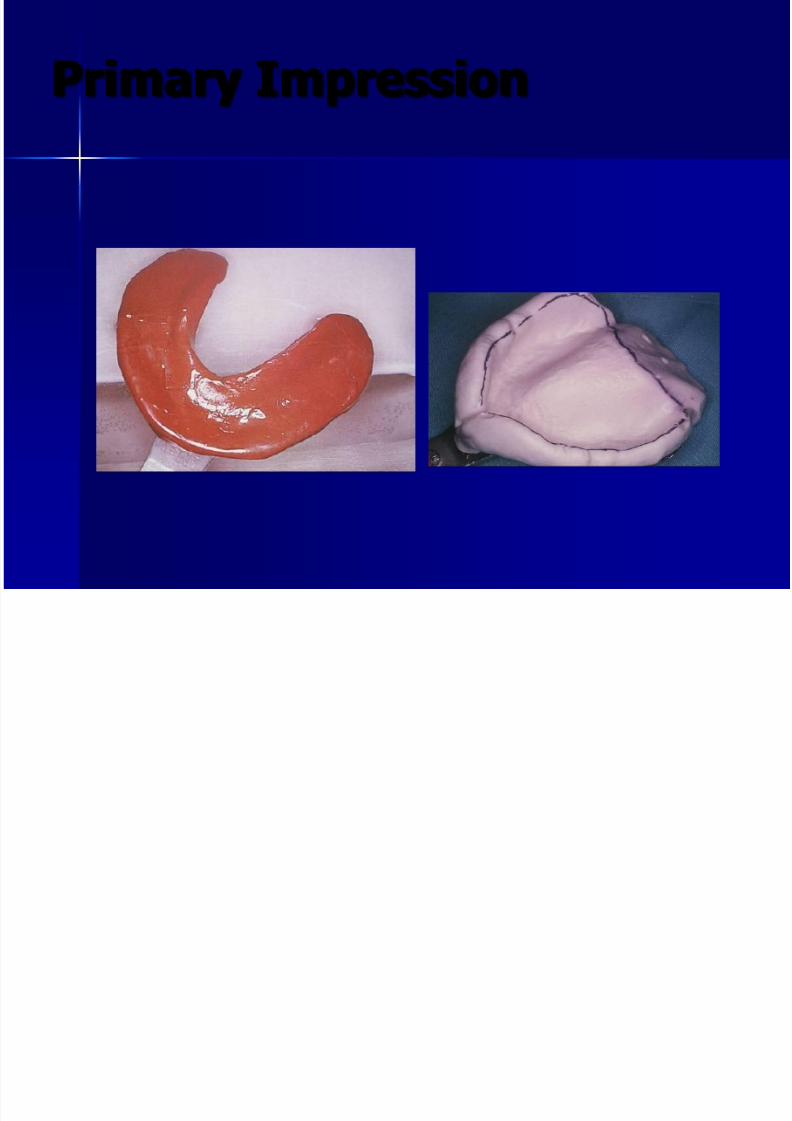
IMPRESSIONS
Impression witha stock tray is
first taken – called a primaryor preliminary
impression
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 17/99
Preliminary
Impressions Impression compound (Modeling
compound
– Thermoplastic Material – - Greatest pressure asserted to the center
of its mass
– Can be softened in wet heat for over- all
adaptation, or it can be softened in small areas by dry heat for localized modifications
– Softening not > 60 C
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 18/99
Preliminary
Impressions Impression compound (Modeling
compound
– Tray selection (cover anatomicallandmarks)
– Kneading of compound to obtain auniform consistency( rope or ball)
– Warming of tray – Adaptation to tray with grooving to
receive crest of ridge( the lingual aspect3mm deeper than labial anteriorly and
6mm posteriorly)
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 19/99
Preliminary
Impressions Impression compound (Modeling
compound
– Can be added and re-adapted
– Used in combination with other materials
– Pouring of impression may be delayed
– Does nor reproduce fine surface details – Should not be used in undercuts
– Re-softening-unhygienic

7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 20/99
IMPRESSION TRAYS
Two types of impressions trays are used – stock and special trays
Properties:
Must be clean and smooth Must be rigid and strong Should permit correct thickness of impression
material to be used (3mm)
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 21/99
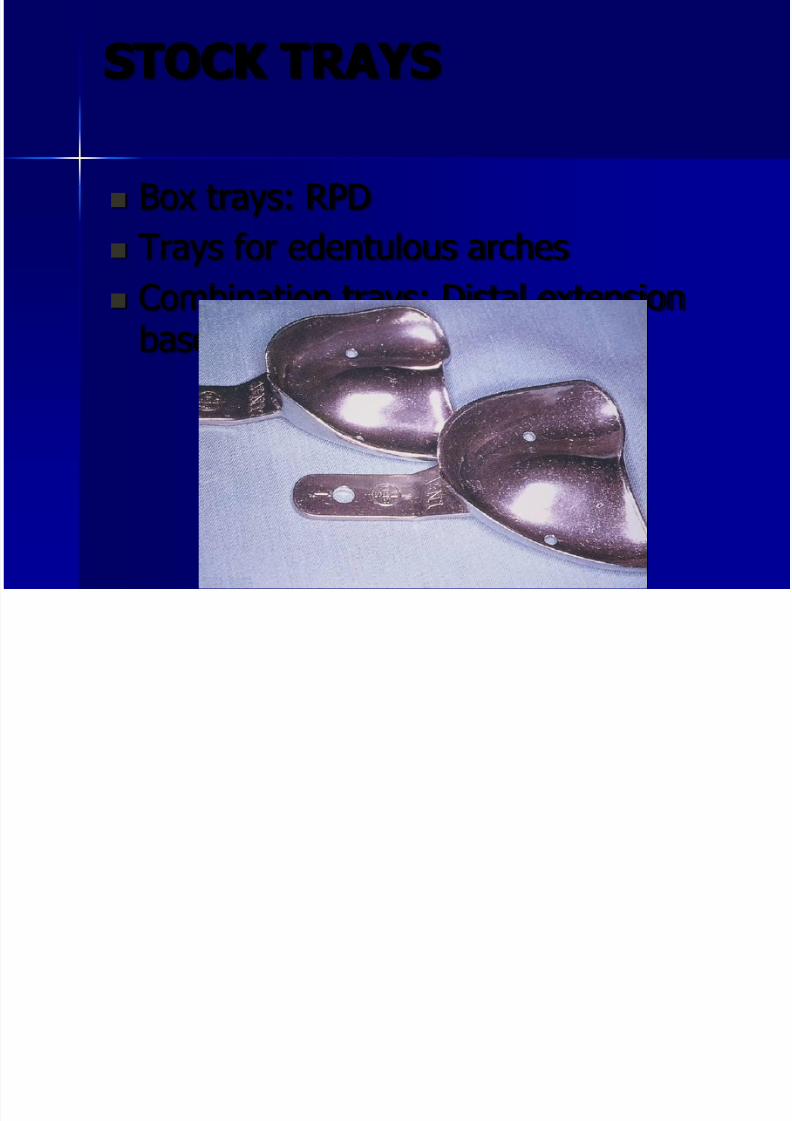
STOCK TRAYS
Box trays: RPD
Trays for edentulous arches
Combination trays: Distal extensionbase

7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 22/99
STOCK TRAYS
Handle must be shaped andattached to the tray so that it
doesn’t displace the lip when theimpression is taken Must hold the impression material in
the correct position in the mouth
and consequently must cover thewhole area of the jaw required inthe impression.
Must prevent distortion of theimpression material during setting
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 23/99
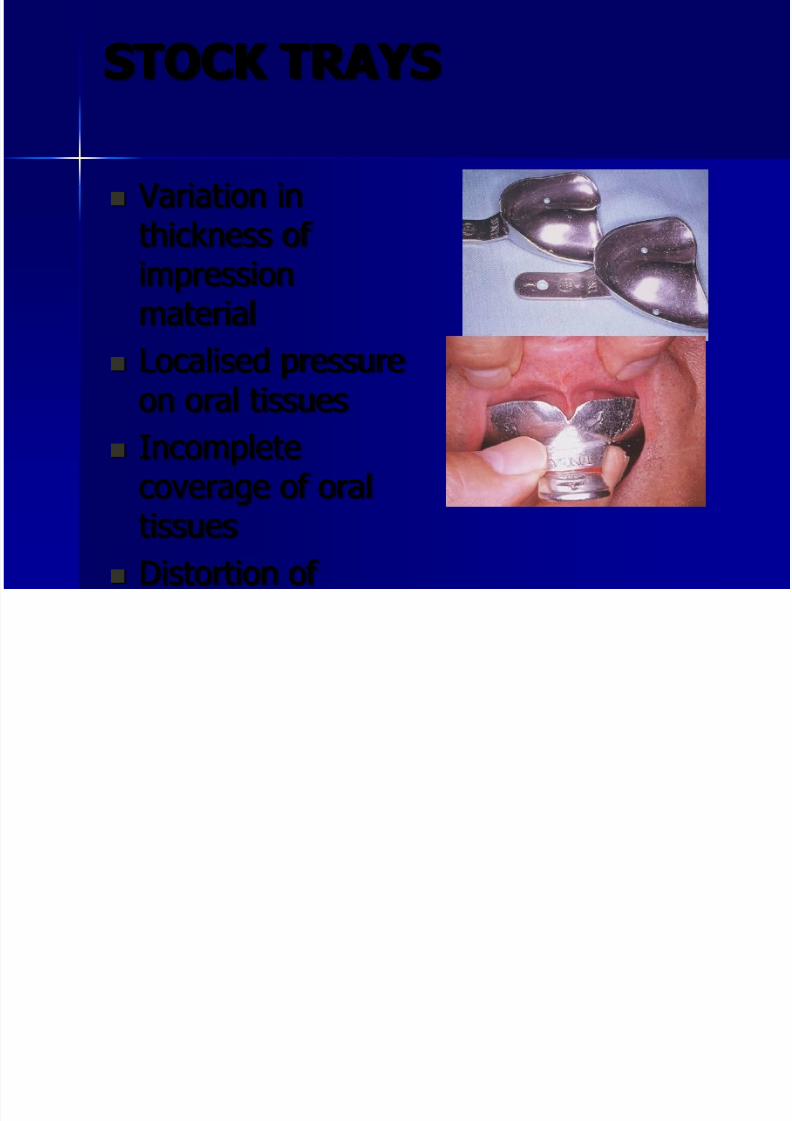
STOCK TRAYS
Variation inthickness of
impressionmaterial
Localised pressure
on oral tissues Incomplete
coverage of oraltissues
Distortion of
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 24/99
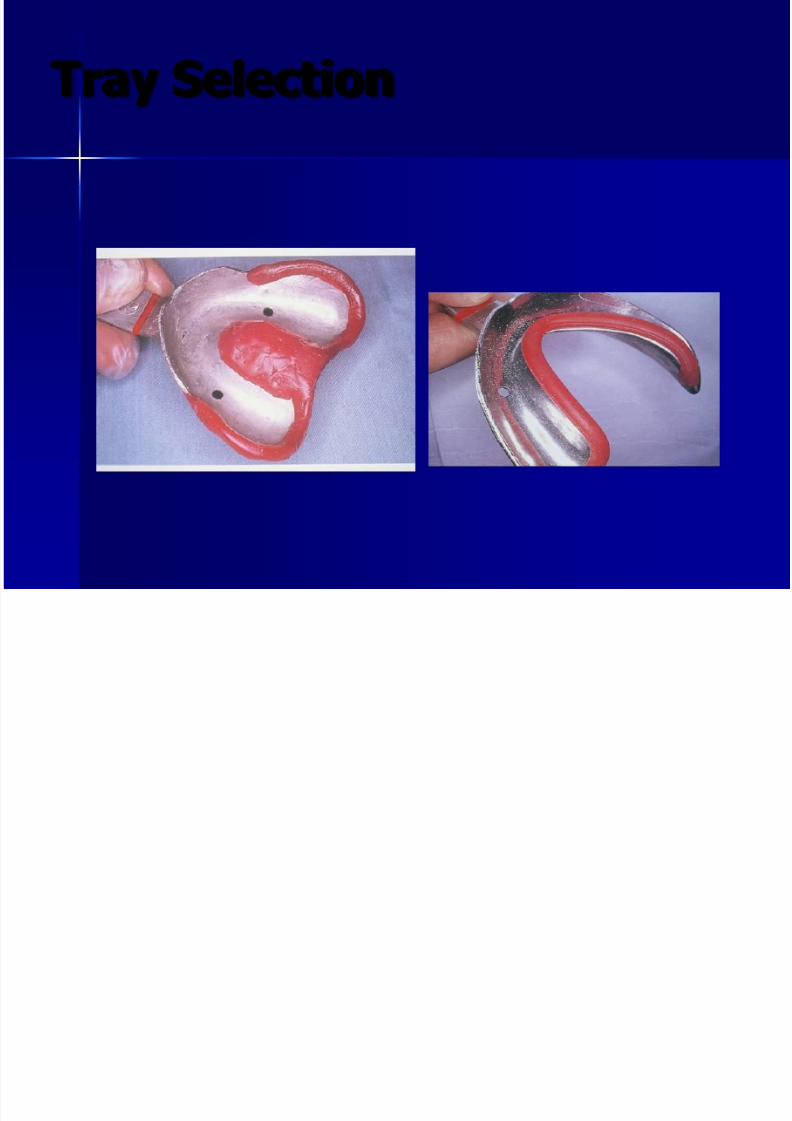
Tray Selection
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 25/99
Primary Impression
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 26/99
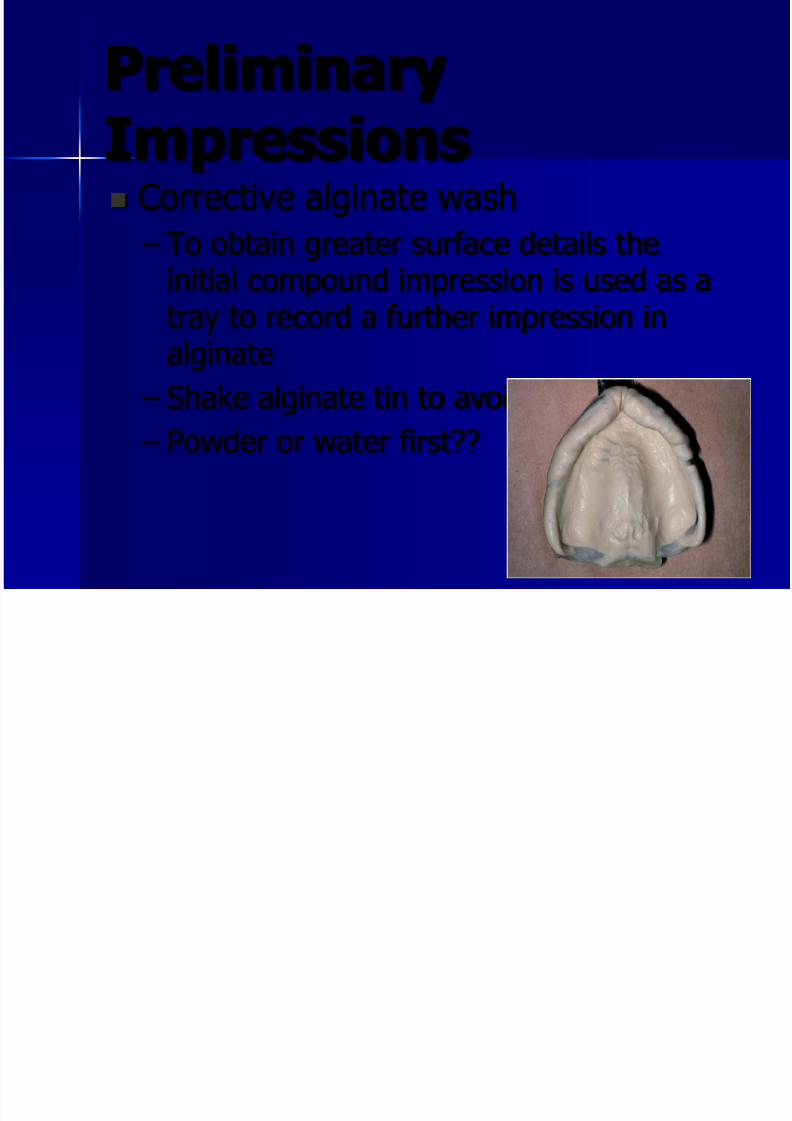
Preliminary
Impressions Corrective alginate wash
– To obtain greater surface details the
initial compound impression is used as atray to record a further impression inalginate
– Shake alginate tin to avoid condensing??
– Powder or water first??
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 27/99
Preliminary
Impressions Alginate
– Sodium alginate, calcium sulphate,
trisodium phosphate – Perforated trays, adhesive( polyamide in
isoprpyl alcohol)
– Impression poured immediately(imbibition and syneresis): 30 minutes
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 28/99
Preliminary
Impressions Alginates
– Record good surface detail with a
minimum of tissue displacement – Accuracy depends upon the accuracy of
the tray
– Easily distorted
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 29/99
Preliminary
Impressions Alginates
– Excellent surface details
– Elastic---undercuts
– Different viscosities
– Not flow in areas not supported by tray
– Cannot be added – Liable to distortion at laboratory
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 30/99
Preliminary
Impressions Maxillary or mandibular impression
first???
– Increase salivation-----Maxillary – Retching reflex---------Maxillary
– Chocking by impression----Maxillary
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 31/99
Preliminary
Impressions Common faults: (lower impression)
– Edge of the tray showing:
Incorrect centring of the tray Use of too large or too small tray
Forward thrust of tongue not been counteredby backward pressure on the tray in the
anterior region
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 32/99
Preliminary
Impressions Common faults: (lower impression)
– Insufficient depth at lingual pouch:
Short flange Lack of compound
Too little force applied
Tongue trapped
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 33/99
Preliminary
Impressions Common faults: (Upper impression)
– Deficiency in midline of palate
Insufficient compound Insufficient pressure
Compound cold
Trapped air
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 34/99
Lab forms
Special trays
– Tray Material
– Amount of spacer and location of tissuestops
– Tray perforations
– Tray handle
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 35/99
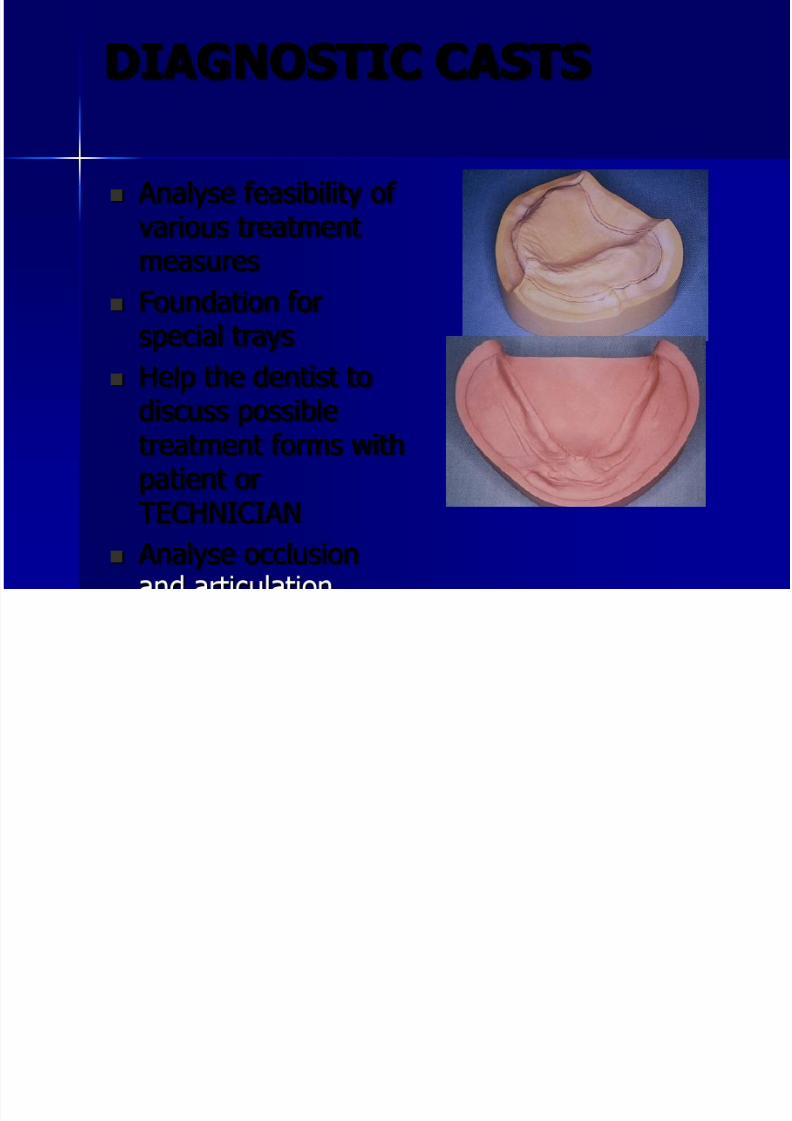
DIAGNOSTIC CASTS
Analyse feasibility of various treatmentmeasures
Foundation forspecial trays
Help the dentist to
discuss possibletreatment forms withpatient orTECHNICIAN
Analyse occlusion
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 36/99
CASTS MATERIAL
Compatible with all types of impression materials
Reasonable setting and working time
Reproduce surface details
Exhibit surface hardness
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 37/99
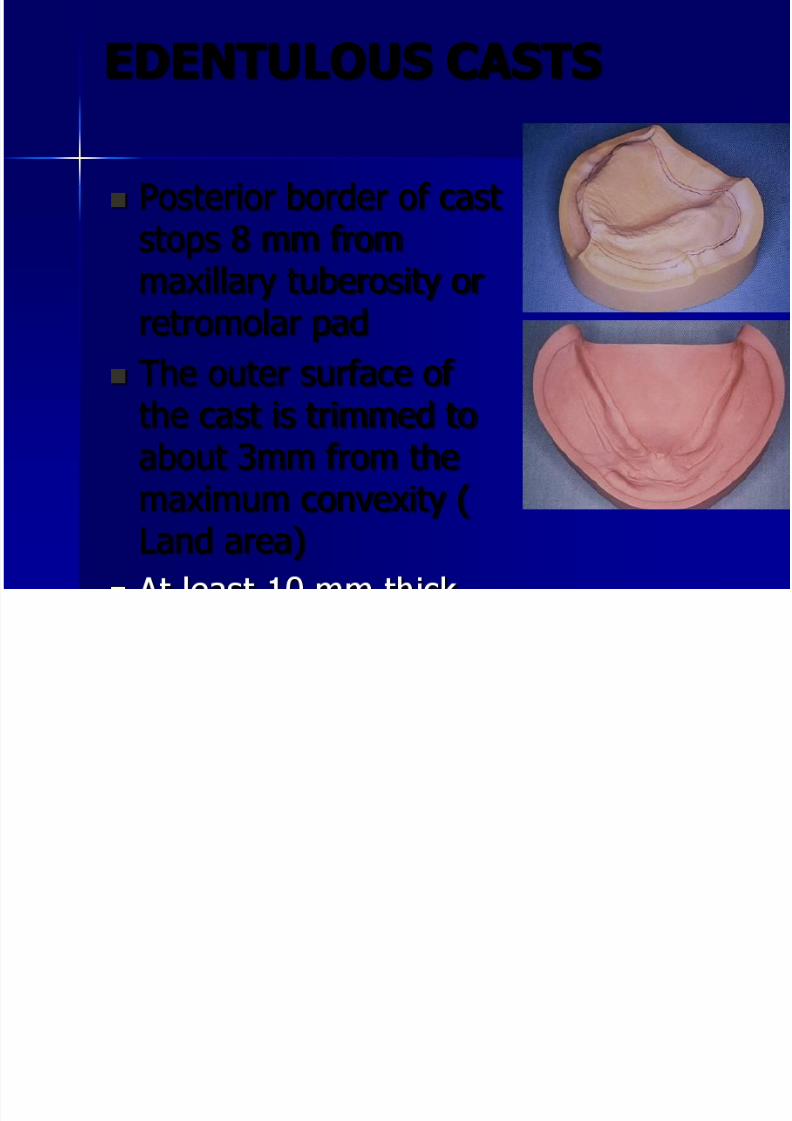
EDENTULOUS CASTS
Posterior border of caststops 8 mm from
maxillary tuberosity orretromolar pad
The outer surface of
the cast is trimmed toabout 3mm from themaximum convexity (
Land area)
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 38/99
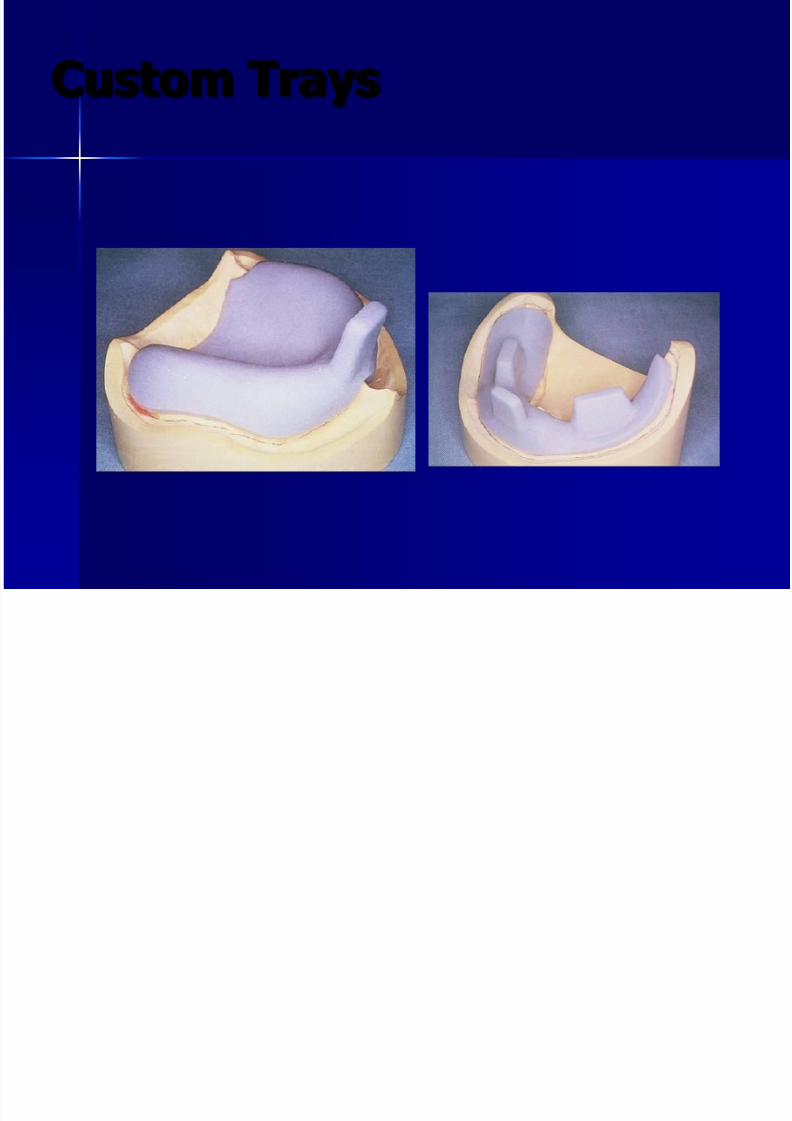
Custom Trays
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 39/99
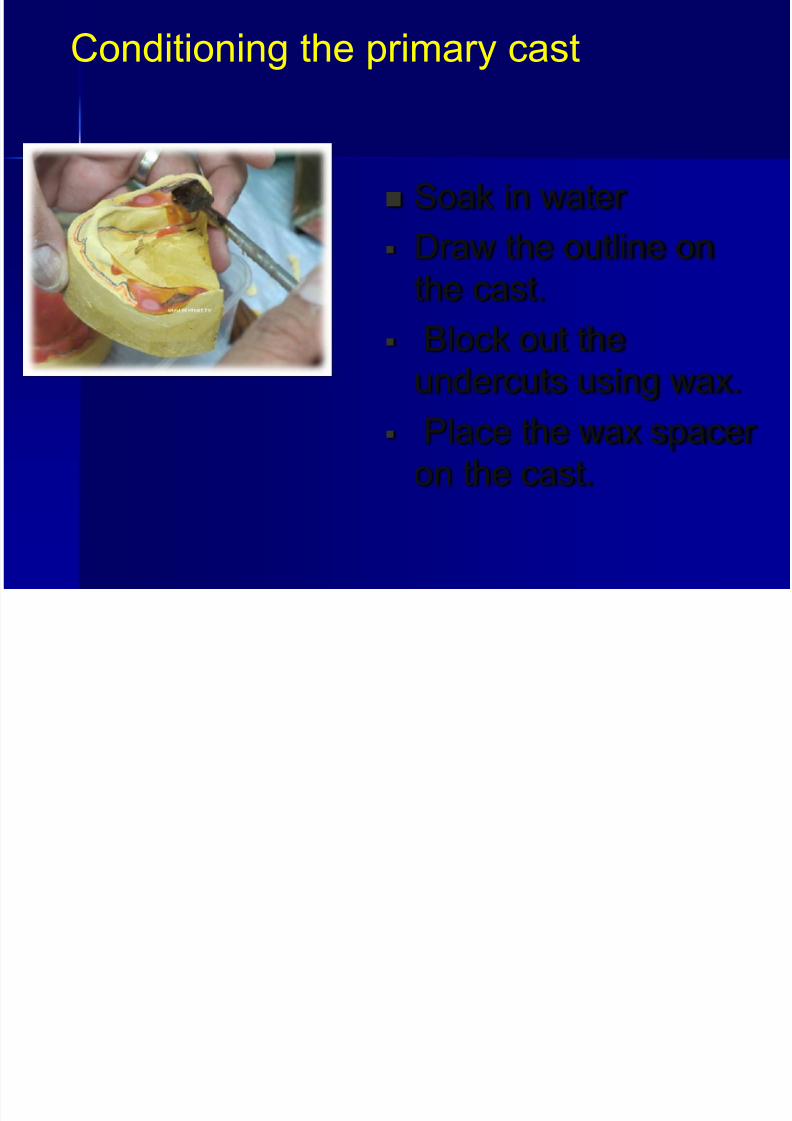
Soak in water
Draw the outline on
the cast.
Block out the
undercuts using wax.
Place the wax spacer on the cast.
Conditioning the primary cast
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 40/99
SPECIAL TRAYS
The special tray can be either spaced orclose fitting.
Spaced trays are used with impressionplaster and alginate. The mould iscovered with a wax spacer and an acrylicsheet of at least 2mm thickness is then
used to construct the tray. If the sheetis too thin, there will be no rigidity thuscausing distortion of the impression.
Close fitting trays are constructed with
the undercuts blocked out on the cast.
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 41/99
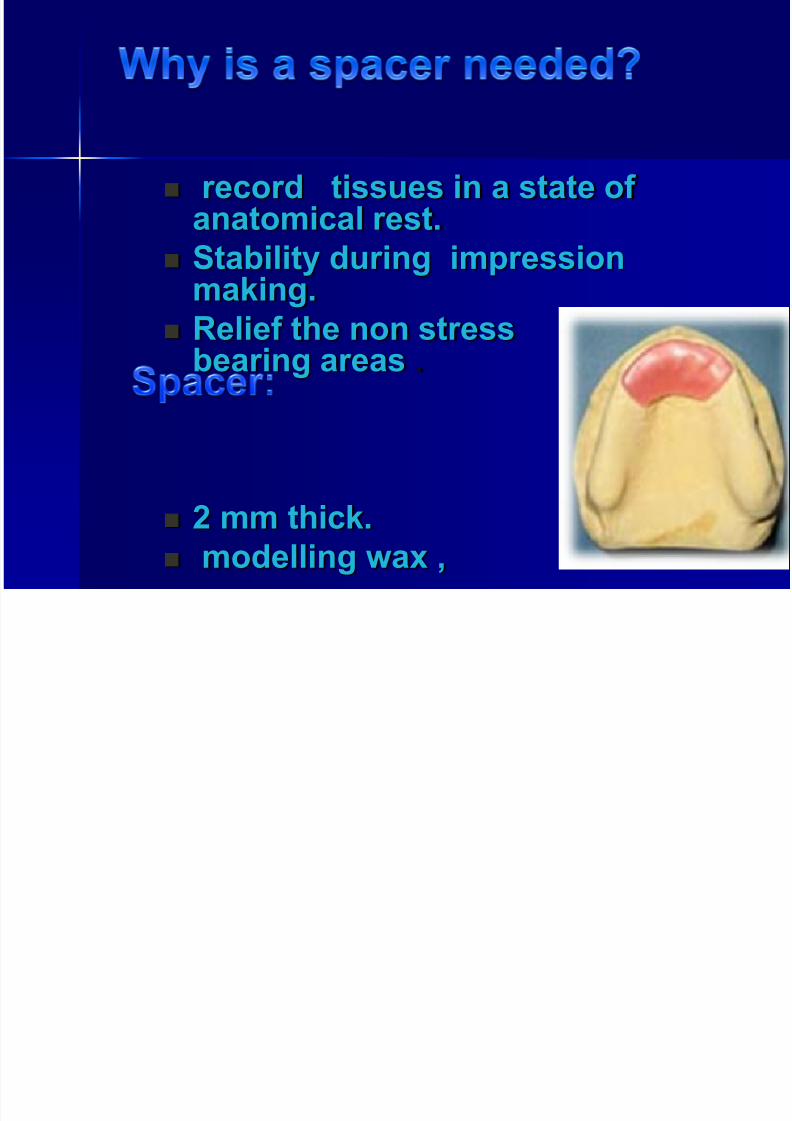
record tissues in a state of anatomical rest.
Stability during impressionmaking.
Relief the non stressbearing areas .
2 mm thick.
modelling wax ,
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 42/99
SPECIAL TRAYS
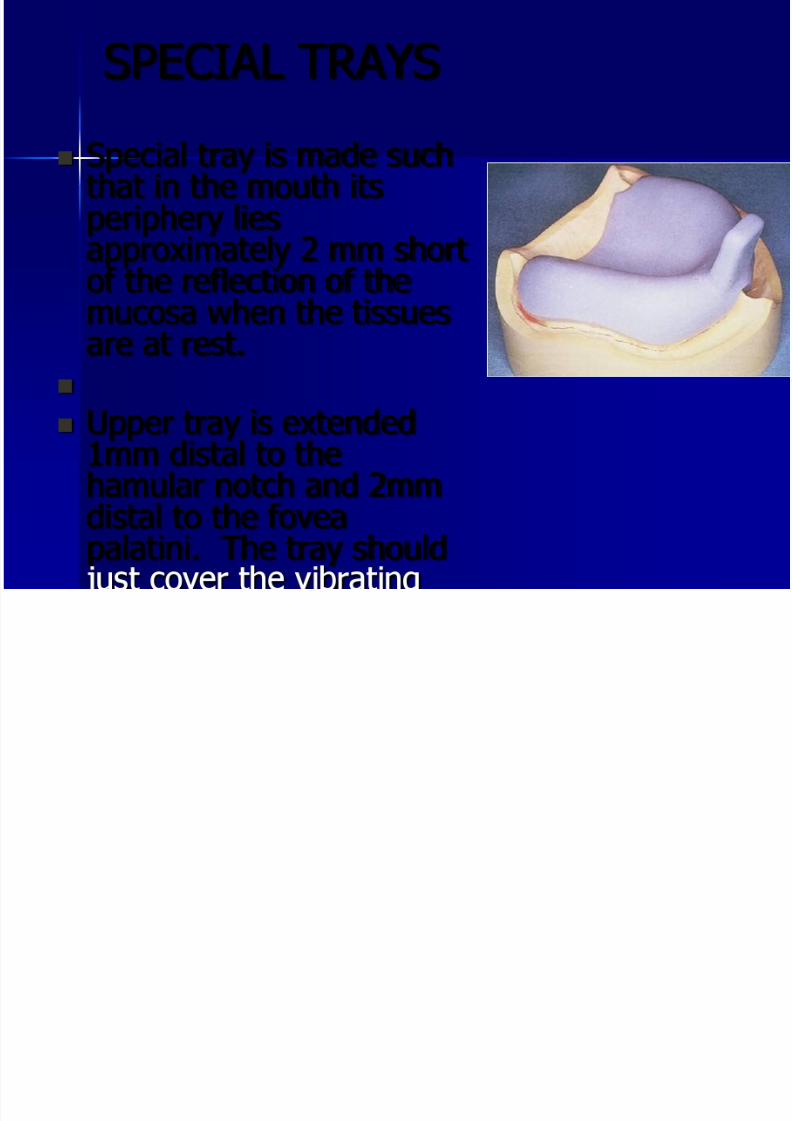
Special tray is made suchthat in the mouth itsperiphery liesapproximately 2 mm short
of the reflection of themucosa when the tissuesare at rest.
Upper tray is extended1mm distal to thehamular notch and 2mmdistal to the fovea
palatini. The tray should
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 43/99
SPECIAL TRAYS
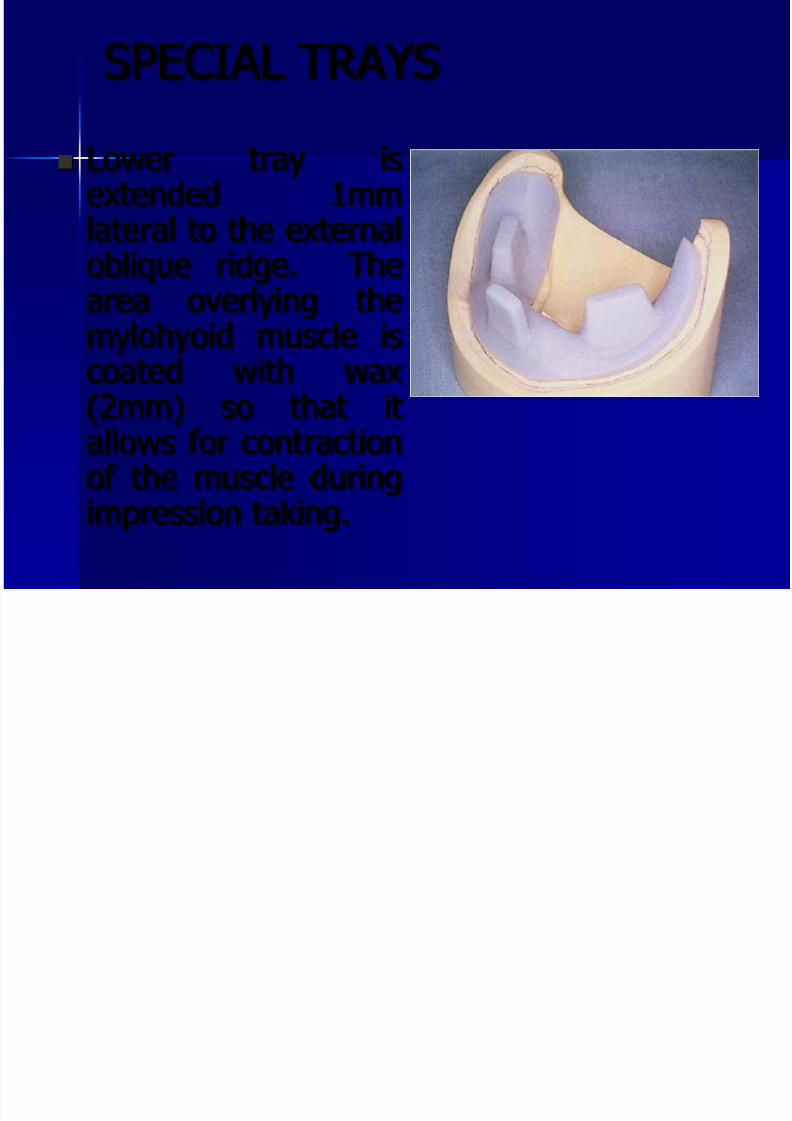
Lower tray isextended 1mmlateral to the externaloblique ridge. Thearea overlying themylohyoid muscle iscoated with wax
(2mm) so that itallows for contractionof the muscle duringimpression taking.
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 44/99
SPECIAL TRAYS
Materials used to construct the trays:
Acrylic resins – can be cold cured or heat
cured. Tray handle position is importantand depending on the impressionmaterial to be used a spacer isincorporated. In addition to the trayhandle finger rests can be incorporatedespecially in the lower and should be1cm long by 1cm high and 4mm wide.
These are usually placed in the lower
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 45/99
SPECIAL TRAYS
To provide the space in the tray for thematerial, the model is covered first with
2 layers of wax and then the trayadapted to the surface.
When alginate is used, holes can bedrilled through the tray to providemechanical retention.
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 46/99
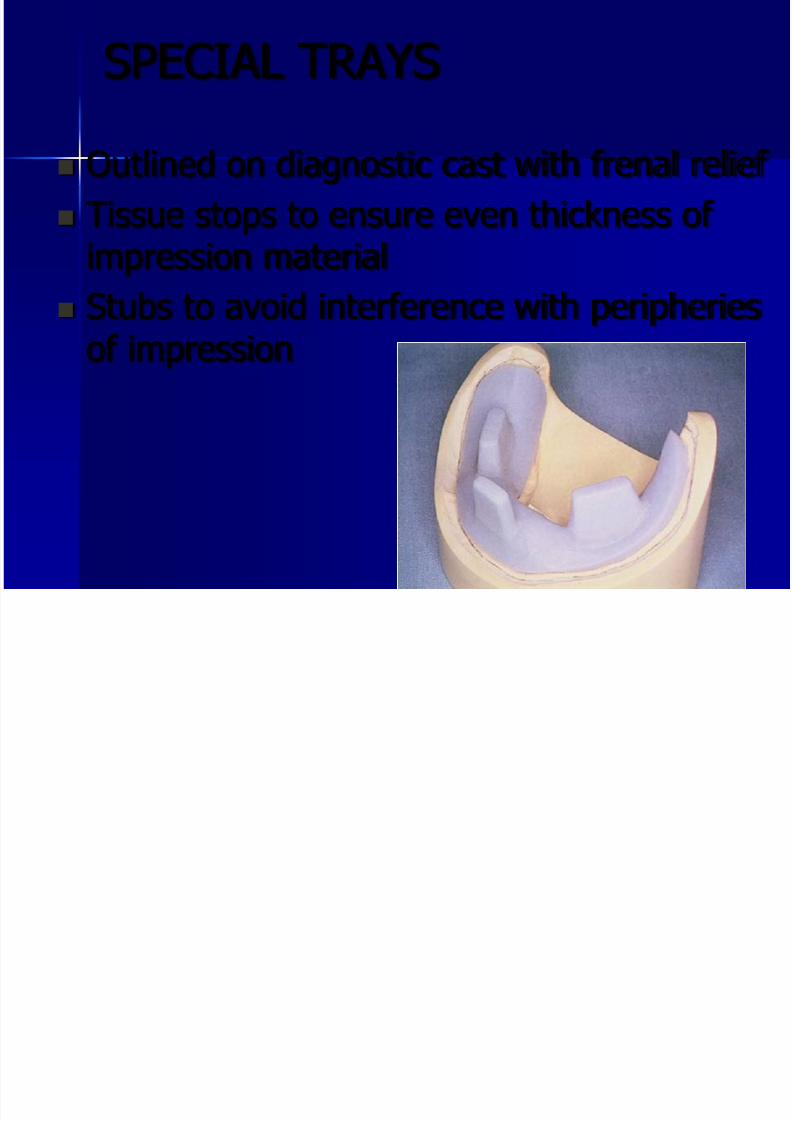
SPECIAL TRAYS
Outlined on diagnostic cast with frenal relief
Tissue stops to ensure even thickness of impression material
Stubs to avoid interference with peripheriesof impression
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 47/99
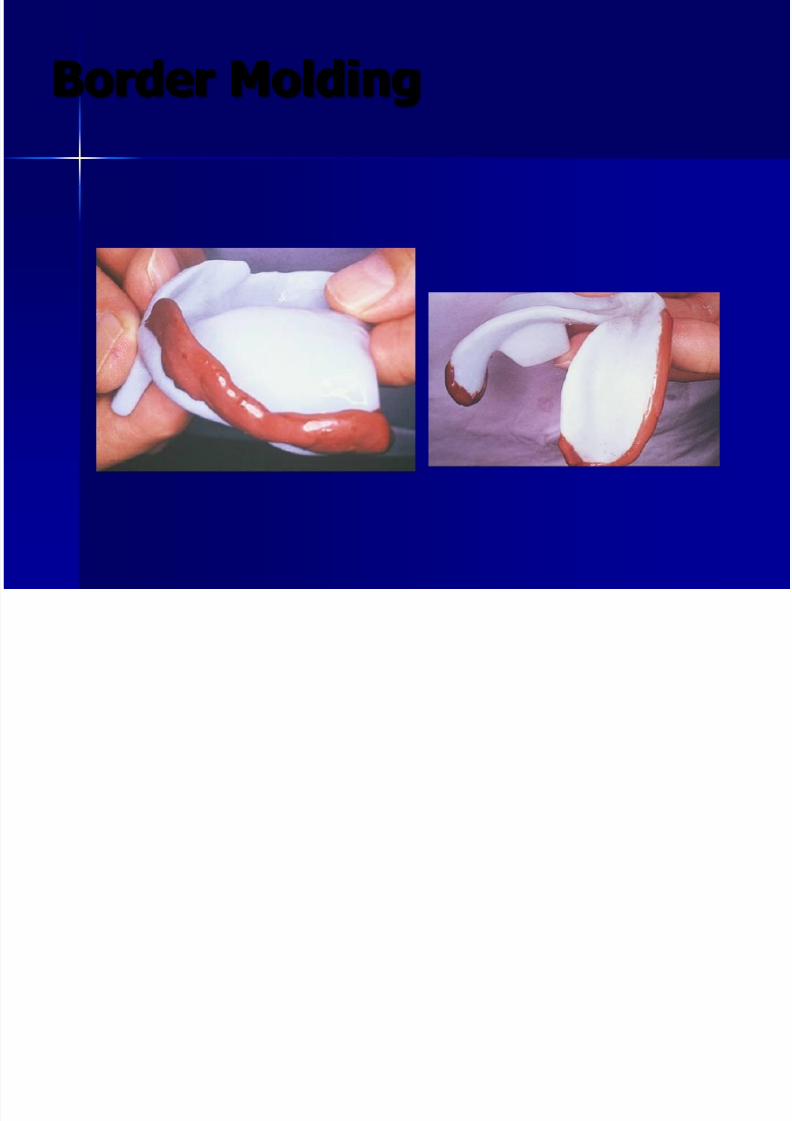
Border Molding
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 48/99
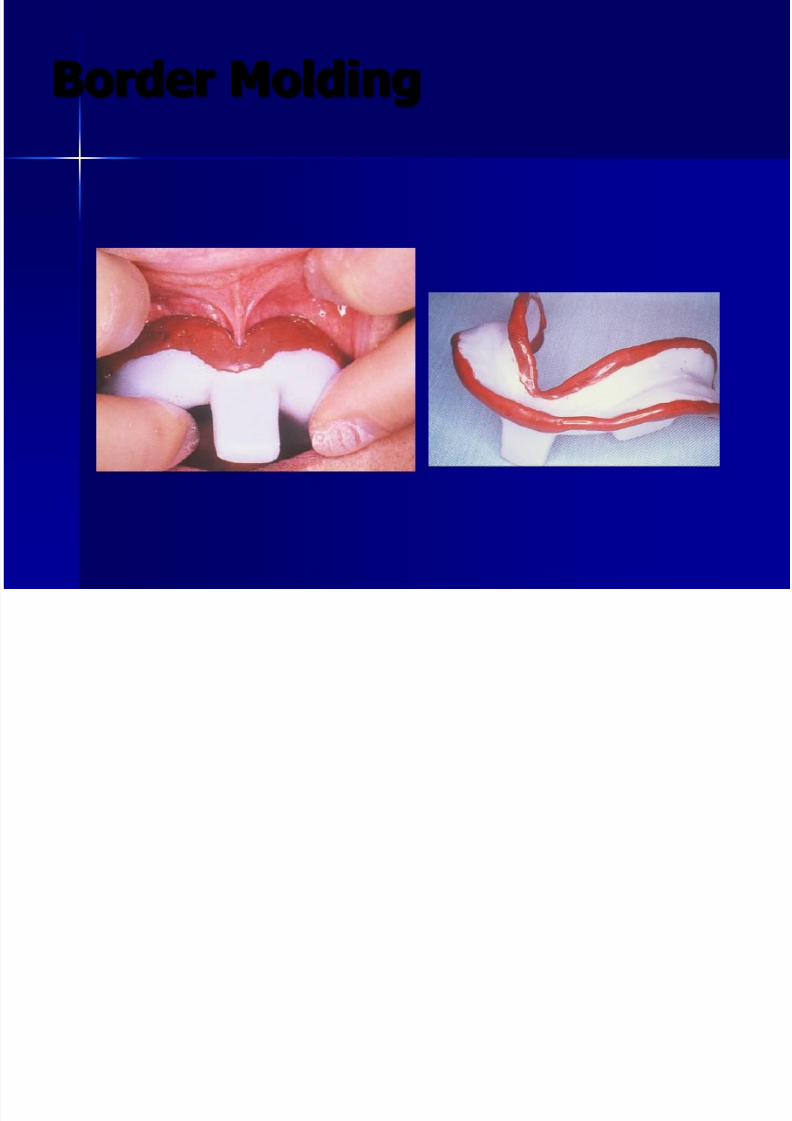
Border Molding
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 49/99
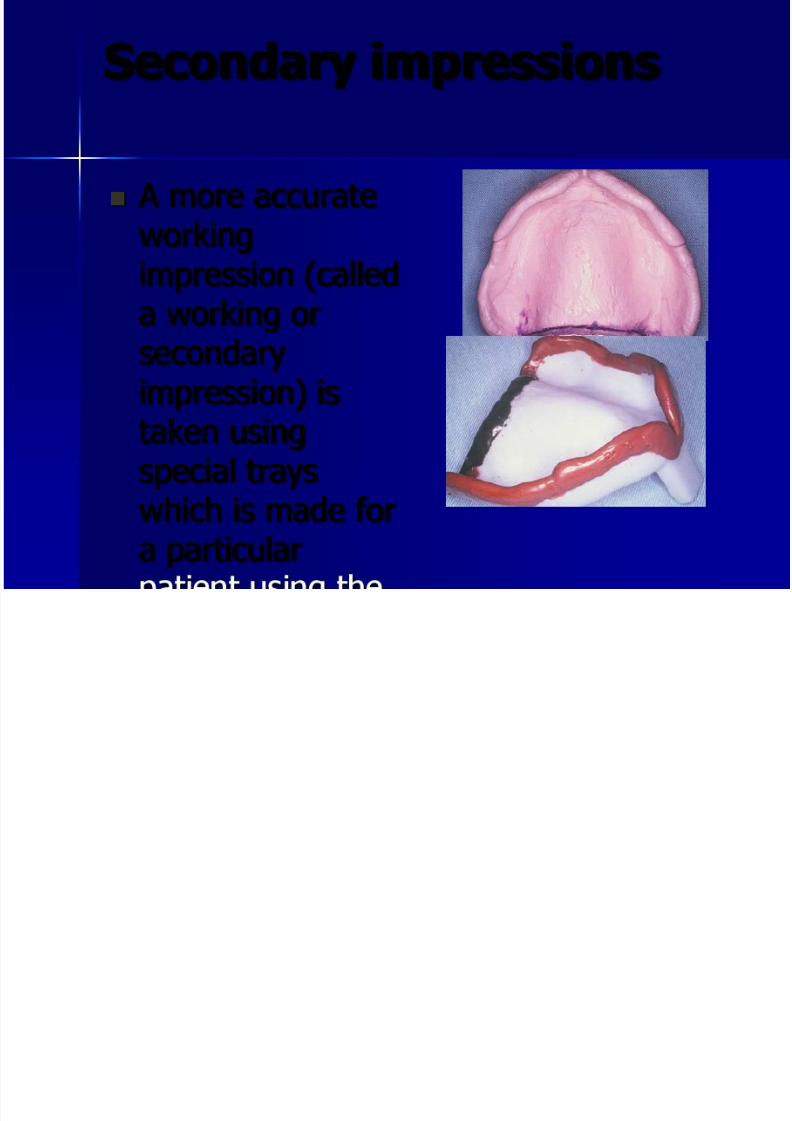
Secondary impressions
A more accurateworking
impression (calleda working orsecondaryimpression) is
taken usingspecial trayswhich is made for
a particular
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 50/99
Secondary impressions
Impression plaster( with anti-expansion liquid)
Zinc-oxide eugenol impression paste(most commonly used)
Alginate
Elastomers (Polysulphides andSilicons)
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 51/99
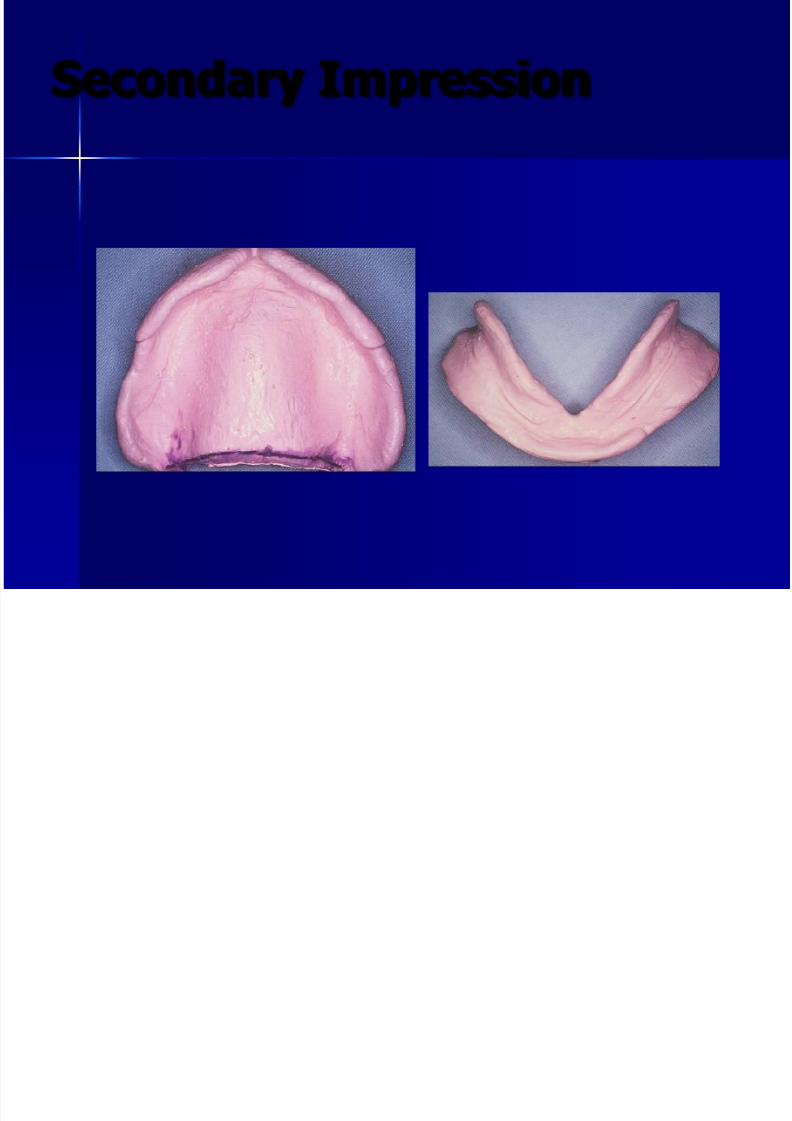
Secondary Impression
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 52/99
Secondary impressions
Zinc-oxide eugenol impression paste
– Composition: Zinc-oxide, white
powdered resin, eugenol, natural oils,fillers.
– Patient lips and nearby skin should belightly covered with facer cream or
petroleum jelly.
– Orange oil or chloroform to remove pastefrom patient or operator skin
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 53/99

7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 54/99
Secondary impressions
Muscle trimming( border moulding).
Aim: to record functional depth and
width of sulcus Using tracing compound-related to--
impression compound???
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 55/99
Secondary impressions
Elastomers
– Polysulphides :
base (polysulphide, titanium dioxide filler) andactivator ( lead dioxide)
Medium body viscosity is used for impression
Hydrophobic material
Prolonged setting time Strong odor of rubber

7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 56/99
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 57/99
IMPRESSION Techniques
Anatomic or arbitrary - Based onlandmarks.
Open or closed mouth - Based on themouth position.
Pressure - Pressure, nonpressure,
negative pressure or selected pressure
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 58/99
IMPRESSION Techniques
Mucocompressive: Displace oraltissues because pressure is needed to
seat the material Mucostatic: No displacement: good
flow properties
Functional: Taken during musclecontraction
Special
7/28/2019 Dr Ziad
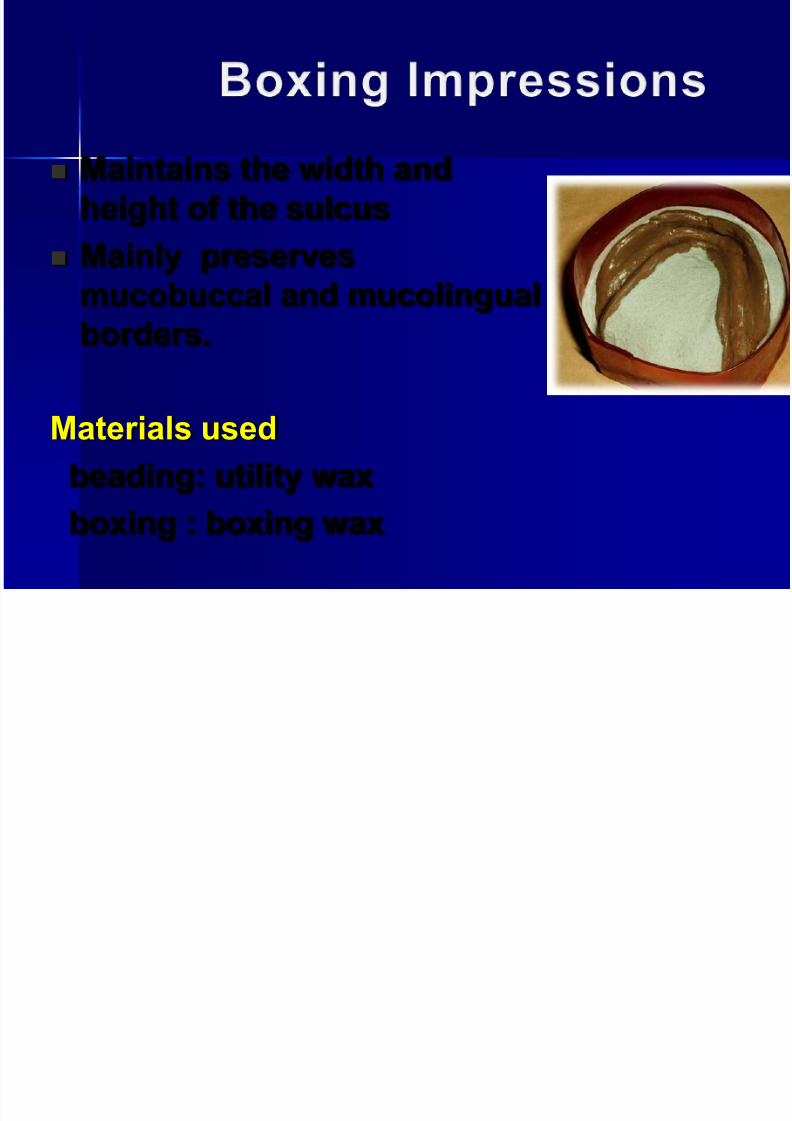
http://slidepdf.com/reader/full/dr-ziad 59/99
Maintains the width and
height of the sulcus
Mainly preserves
mucobuccal and mucolingualborders.
Materials used
beading: utility wax
boxing : boxing wax
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 60/99
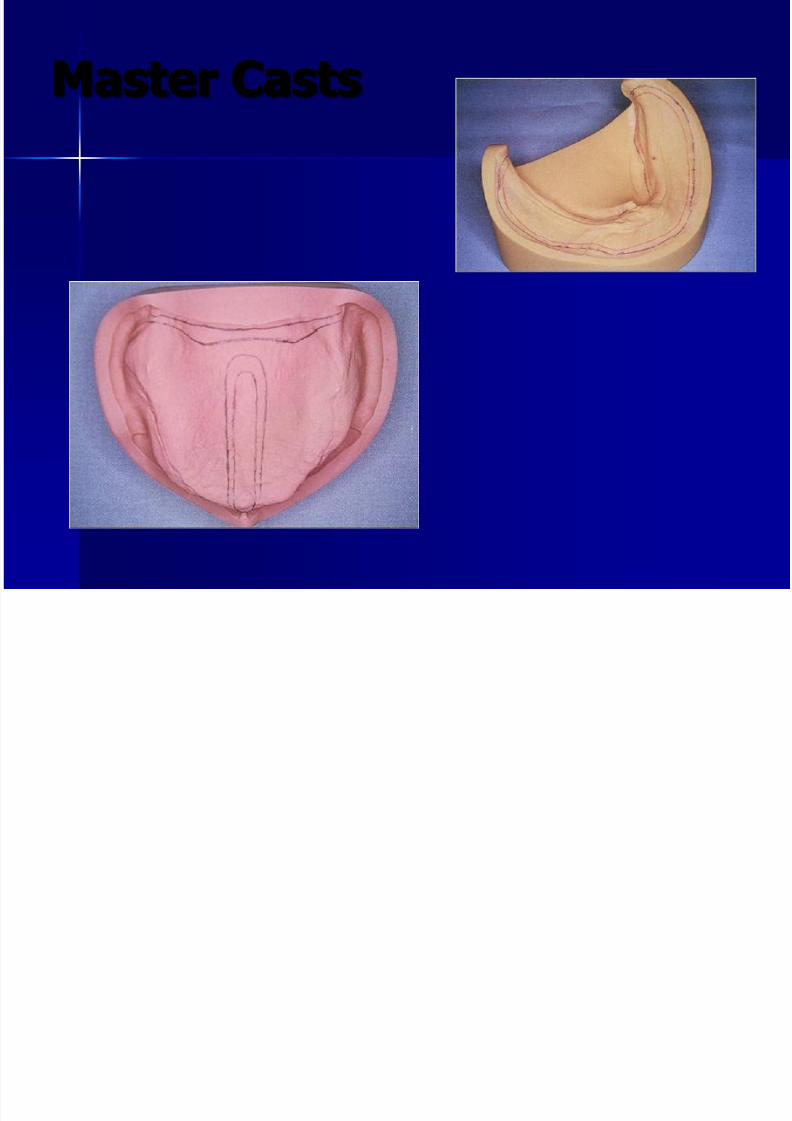
Master Casts
D b
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 61/99
Denture bases
Requirements
– Easy to handle
– Capable of reproducing details from cast – Should not distort at mouth temperature
– Capable of being modified at chairside
Made of: wax, shellac, acrylic resinand impression compound
D b
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 62/99
Denture bases
Acrylic resin (heat cure, self-cured, lightcured) bases have superior fit and stability
Wax bases tend to distort if left in mouth orif subjected to heavy occlusal forces
Shellac is more stable than wax but difficultto adjust at the chairside
Compound bases may be used in caseswhere the rim is to be made of the samematerial
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 63/99
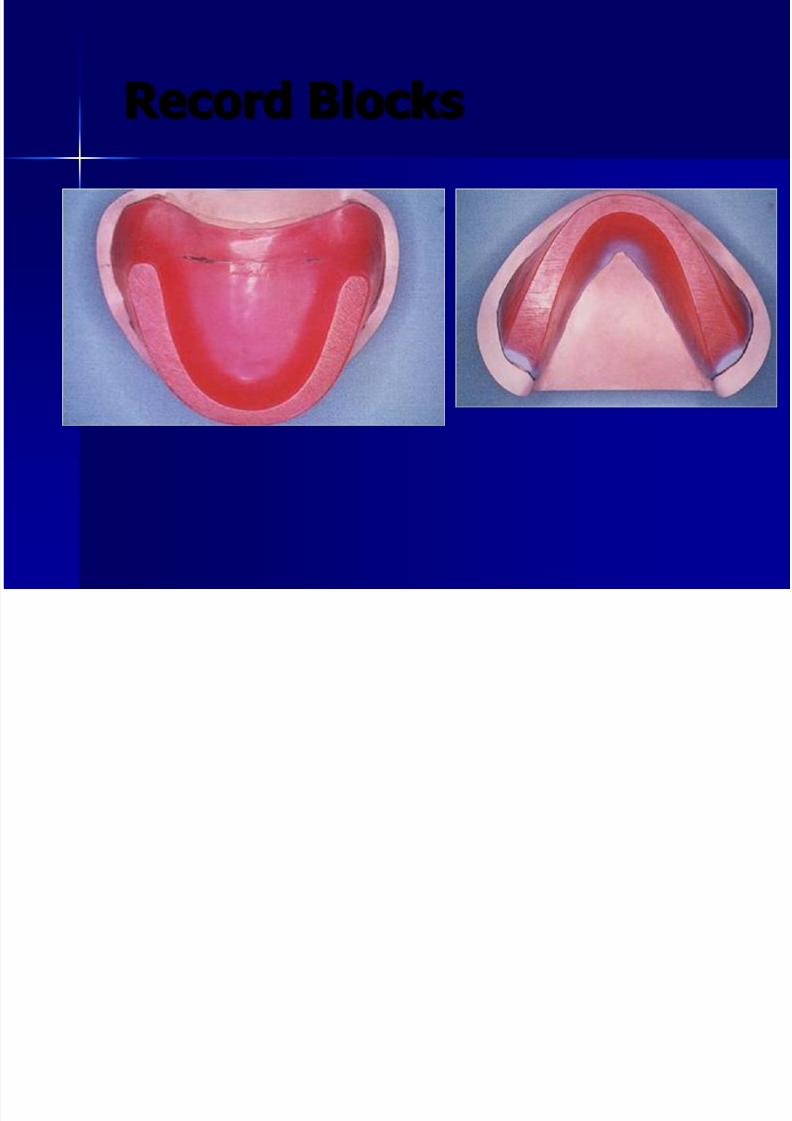
Record Blocks
Record base
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 64/99
Record base
Base of denture Support wax occlusal rims.
Requirements :
Well adapted to the final cast . Dimensionally stable.
Retentive .
1mm thick on the crest andfacial slope of the ridge .
2mm thick in the palatal andlingual flange.

7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 65/99
Occlusal rims
Occluding surfaces built on temporaryor permanent denture bases for the
purpose of making maxillo-
mandibular relation records andarranging teeth.
o Primarily serves as gingivao Done mainly to arrange teeth
A t i l i f ti
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 66/99
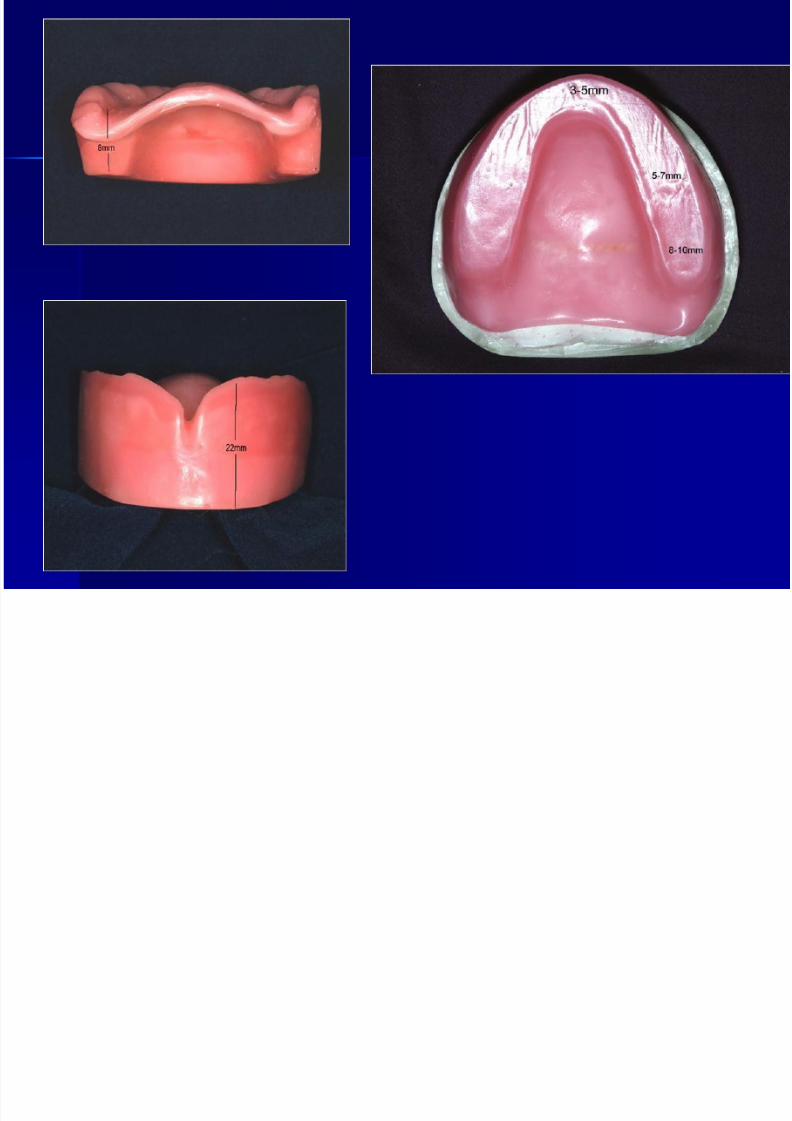
Anatomical information:Maxilla
The labial surface of anterior teethsupport the lips and is between 10 -12mm labial to incisive papilla
The centre of the last molar is nearlyopposite the centre of the tuberosity andits buccal surface is 3-5mm buccal to
centre of tuberosity On average, the distance from the
functional sulcus to incisal edge of centrals is about 20mm and to the
occlusal surface of first molar is about
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 67/99
22mm high from the depth of thesulcus.
Ant region should be 8mm away from
incisive papilla .
4 – 6 mm wide in ant region.
Occlusal table should be 18mm high
from the depth of sulcus.
Occlusal table should be 8 –
12 mmwide posterior.
Occlusal table should be 10 – 12 mm
above the crest of alveolar ridge
anteriorly.
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 68/99
A t i l i f ti
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 69/99
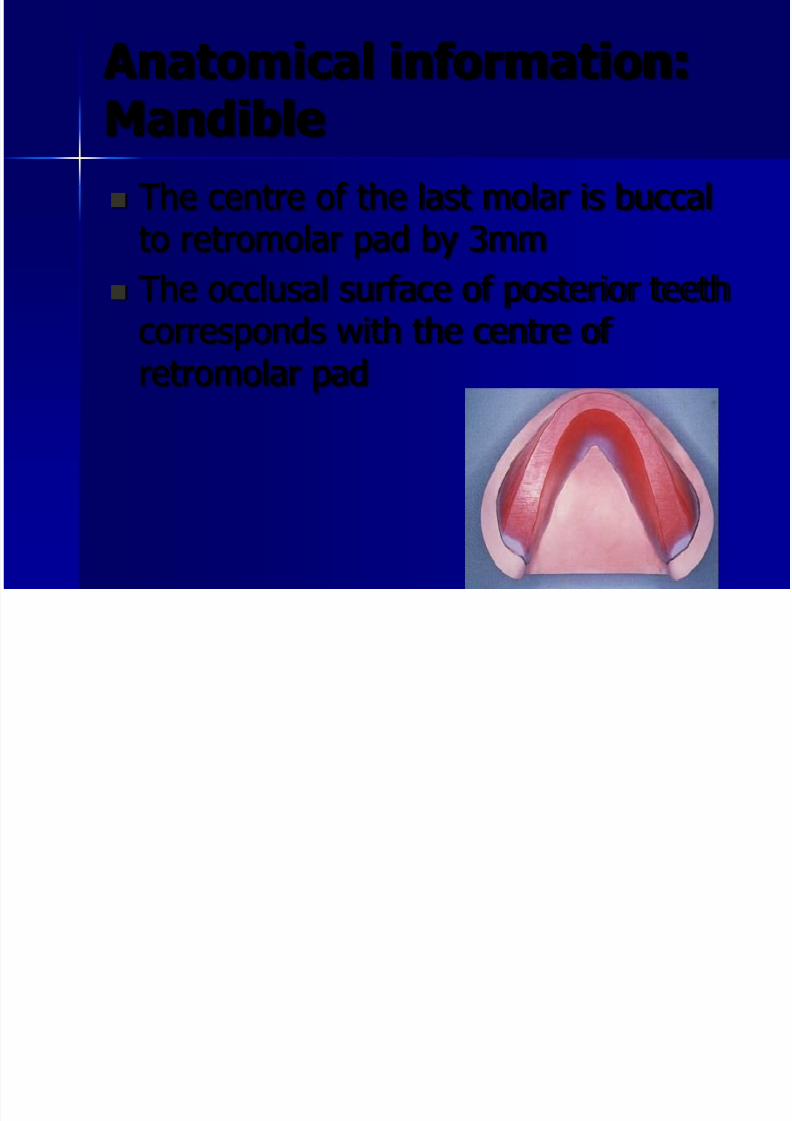
Anatomical information:Mandible
The centre of the last molar is buccalto retromolar pad by 3mm
The occlusal surface of posterior teethcorresponds with the centre of retromolar pad
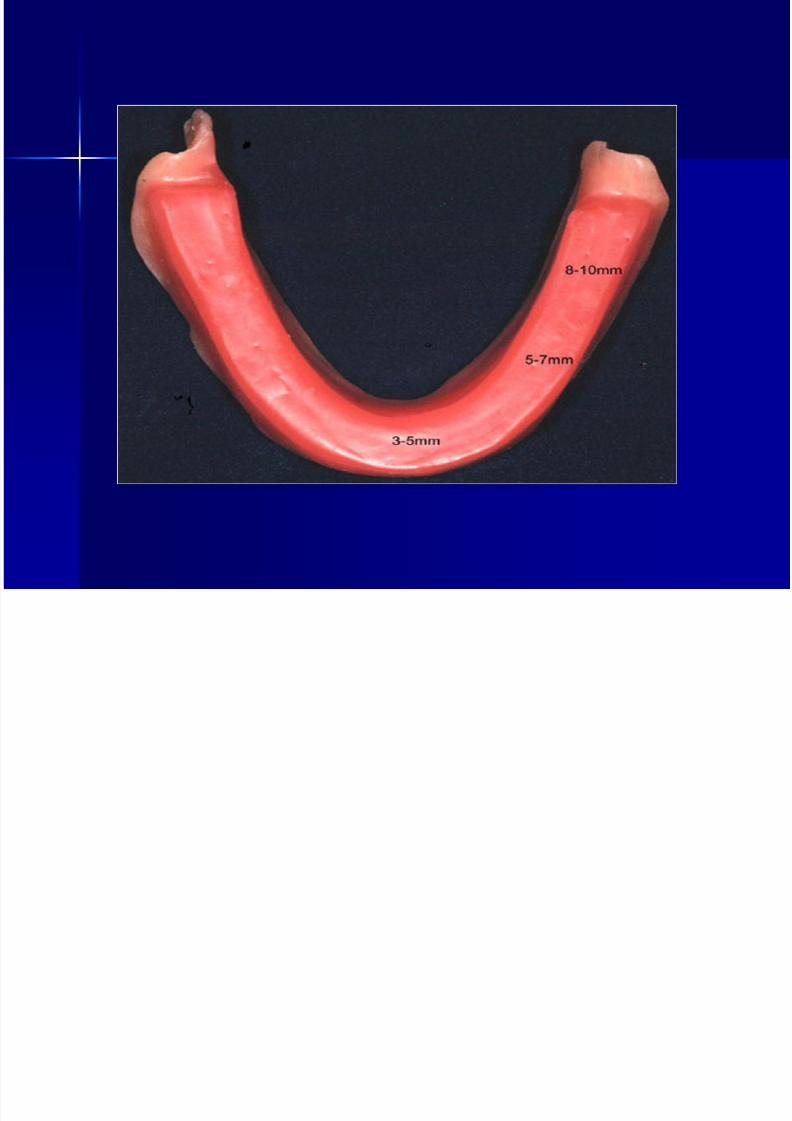
Mandibular occlusal rim
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 70/99
6 -8mm high from the crest of the ridgeanteriorly
18mm high from depth of the sulcus in the
canine eminence region
3 –
6mm high from the crest of the ridgeposteriorly
The occlusal plate should extend to 2/3rd ht of
the retromolar pad posteriorly
Width
anteriorly 4 – 6mm
posteriorly 8 – 12mm

7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 71/99
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 72/99
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 73/99
JAW RELATIONS AND ARRANGEMENT OF ARTIFICIAL TEETH FOR
COMPLETE DENTURES
Jaw relations
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 74/99
Jaw relations
A cast records details of natural dentition andalveolar ridges but we need to know the
following information before denture constructionso that the patient can get the maximum benefitfrom the complete denture:
– Centric occlusion: Static tooth contacts inmaximum intercuspation (termination of masticatory closure).
Jaw relations
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 75/99
Jaw relations
– Centric relation: most retruded position of mandibleto maxilla from which lateral movement can be
made at a given degree of jaw separation.
– Vertical dimension: the distance between alveolarprocess of maxilla and mandible in centric relation
– Occlusal plane: the position and angle of a plane towhich the occlusal surfaces of teeth relate
Jaw relations
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 76/99
Jaw relations
When teeth are missing, theirpositions are taken by record blocks
and these information recorded onthem
The blocks are attached to a base
constructed to accurately fit themouth
Registration blocks( base and wax
rim)
Jaw relations
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 77/99
Jaw relations
Orientation relation: relation to the cranium
Vertical relation: amount of jaw separation
Horizontal relation: antero-posterior andlateral relations
These relations are transferred from patient tocasts (replica of edentulous ridges) throughthe use of: – Face bow( Orientation relation)
– Record blocks( Vertical and Horizontal relations)
Jaw relations
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 78/99
Jaw relations
The established recorded jaw relationsare transferred to a mechanical
instrument that represents TMJ andJaws to which the maxillary andmandibular casts are attached. This isthe articulator which aims to simulatesome or all mandibular movements
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 79/99
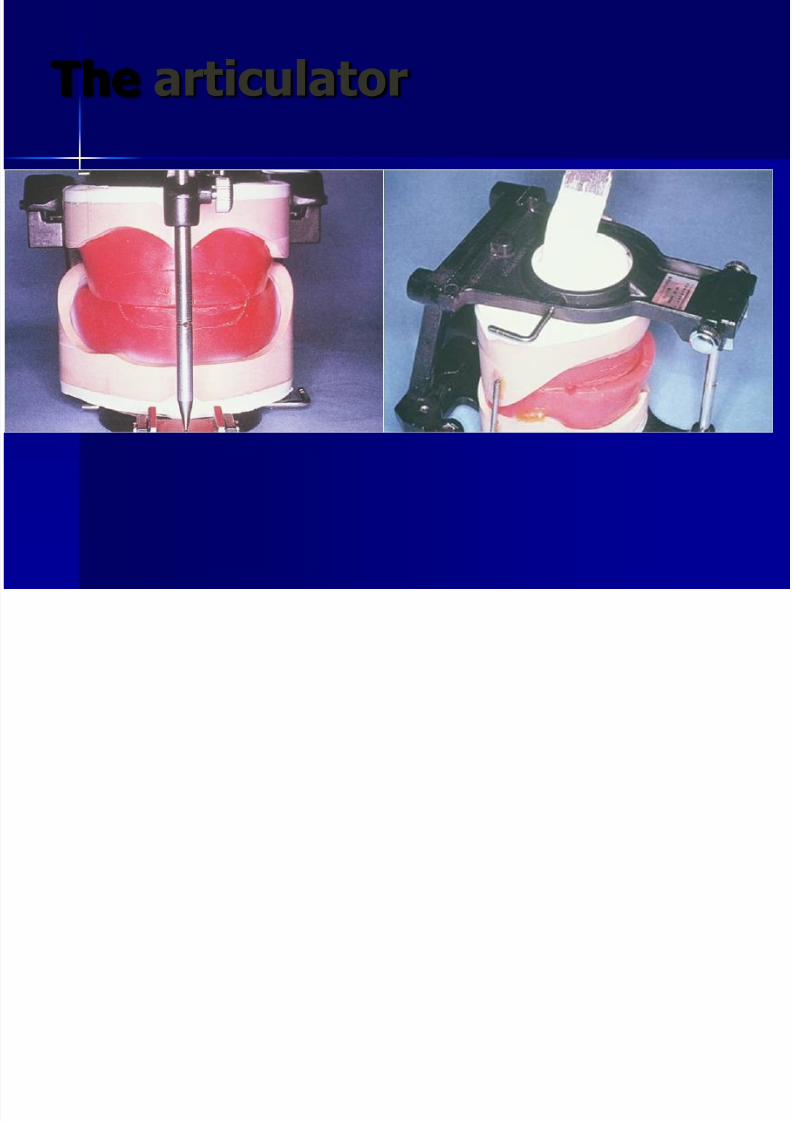
The articulator
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 80/99
Jaw relations
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 81/99
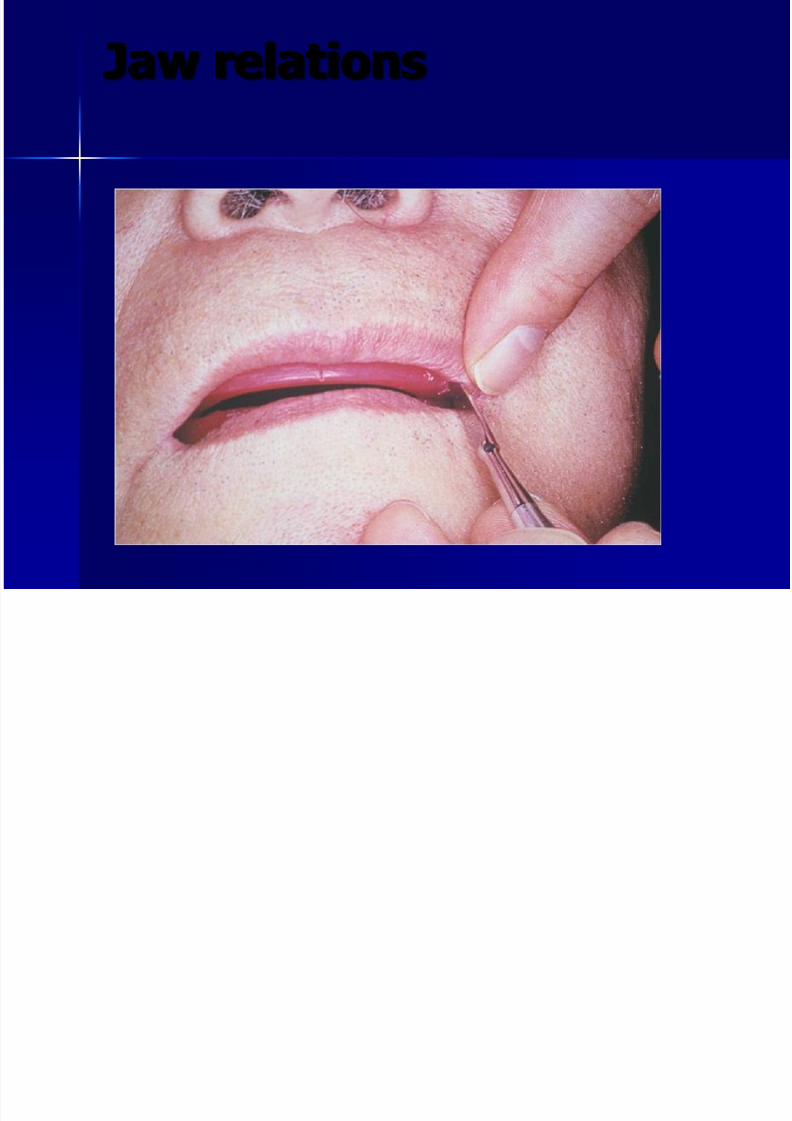
Jaw relations
– Assess lip support and notice vermillionborder and naso-labial groove
– Check height and orientation of occlusalplane( anterior and antero-posterior): thelower border of the maxillary rim represents thelevel at which the incisive edge of the upper
central incisors will be set and decides howmuch of the incisal edge will be seen below themargin of upper lip( 1mm average)
Jaw relations
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 82/99
Jaw relations
Jaw relations
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 83/99
Jaw relations
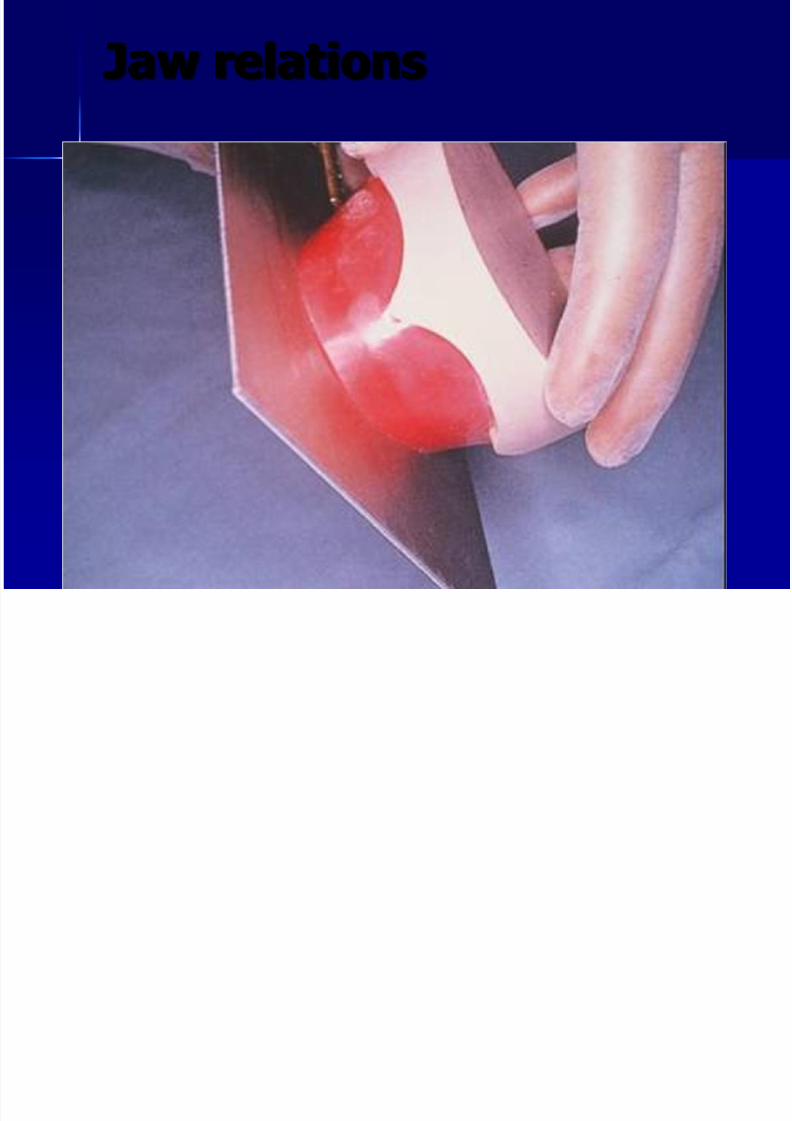
Maxillary rim
– Check height and orientation of
occlusal plane( anterior and antero-posterior
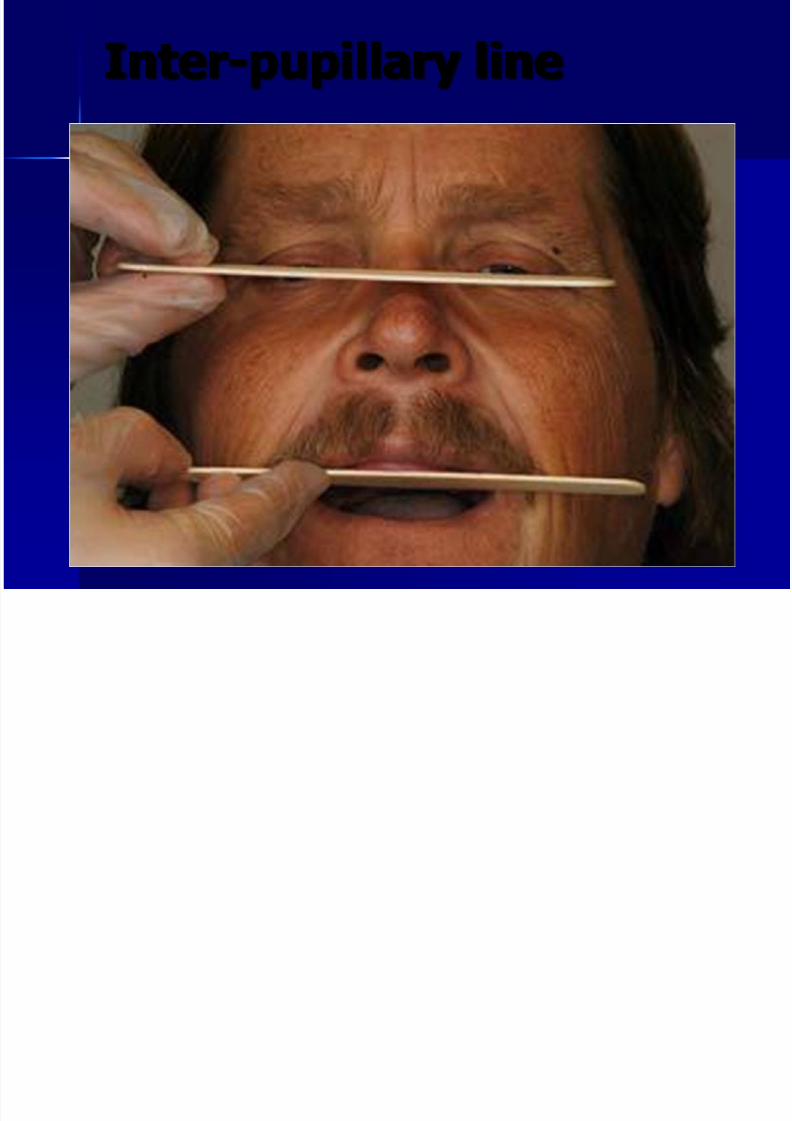
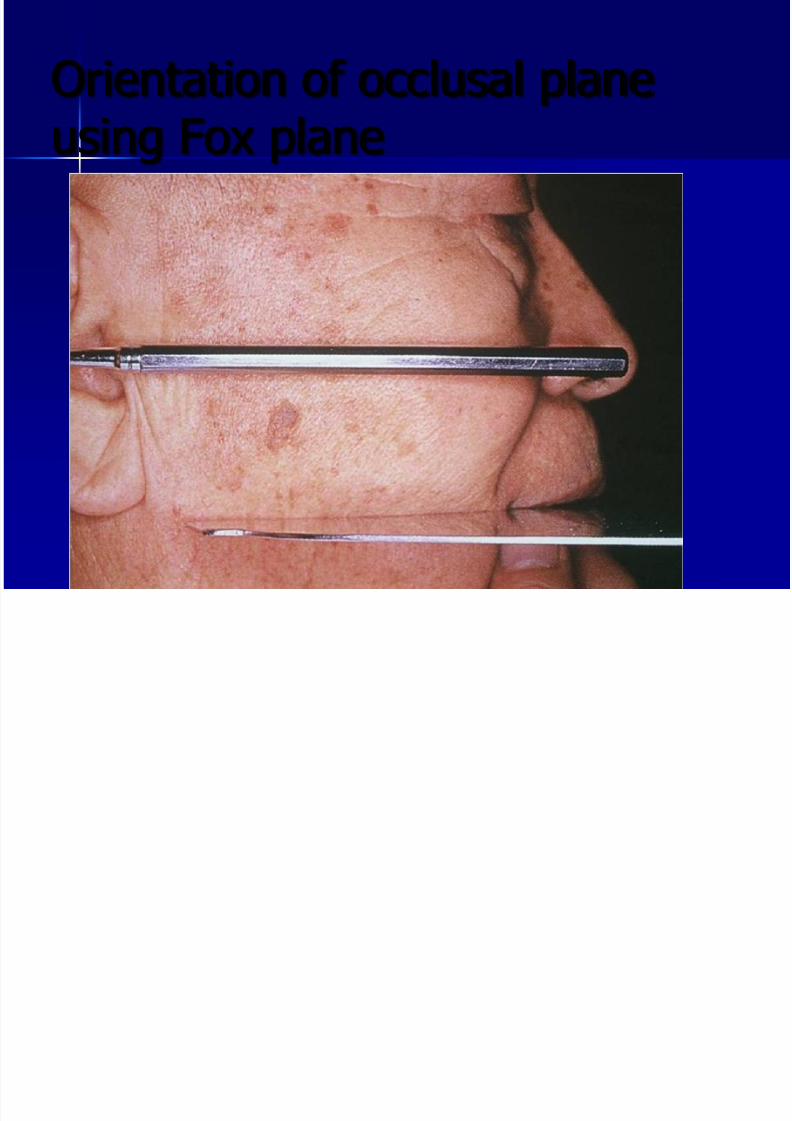
– the anterior occlusal plane is trimmedparallel to the inter-pupillary line while
the patient is in rest
– The antero-posterior plane is parallel toCamper’s line( ala-tragus line)
Inter-pupillary line
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 84/99
Inter-pupillary line
O i i f l l l
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 85/99
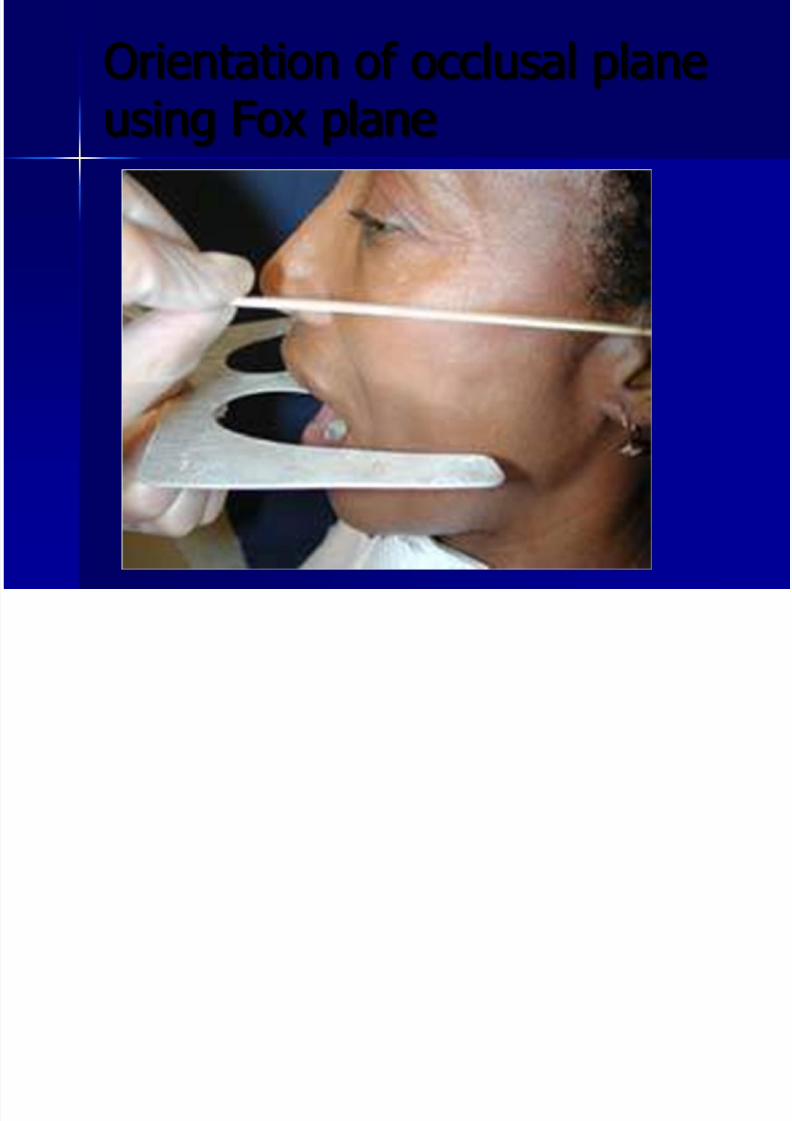
Orientation of occlusal plane
using Fox plane
Orientation of occlusal plane
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 86/99
Orientation of occlusal planeusing Fox plane
Jaw relations
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 87/99
Jaw relations
Maxillary rim
– Check height and orientation of
occlusal plane( anterior and antero-posterior :Mark centre line on labialsurface of upper rim which shouldcorrespond to the centre line of the whole
face and is not necessarily the centre of lips, nose , or any other individual facialstructure
Jaw relations
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 88/99
Jaw relations
Maxillary rim
– Canine lines: better to indicate distal
surfaces of canines – High lip line:
indicates the position of maximum elevation of upper lip when smiling
Assist in selecting length of upper anteriors
Jaw relations

7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 89/99
Jaw relations
Jaw relations
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 90/99
Jaw relations
Jaw relations
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 91/99
Jaw relations
Maxillary rim
– Measure rest vertical dimension
– Patient seated upright with Frankfurtplane horizontal (lowest point in marginof orbit to highest margin of externalauditory meatus).
– Ask patient to relax:
Swallow and relax
Pronounce ‘em’ and relax
Moisten lips with tip of the tongue and relax
Jaw relations
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 92/99
Jaw relations
Maxillary rim
– Measure rest vertical dimension
(VDR) – The VDR is measured using
Willis gauge: separation between lower borderof nasal septum and lower border of chin (
pressure applied and angulations of gaugemay differ
2-dot technique: most common: tip of the
nose and non-movable part of chin)
2-dot technique

7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 93/99
2 dot technique
Jaw relations
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 94/99
Jaw relations
Measure Occlusal verticaldimension (VDO):
– Insert lower base plate and wax rim – Ensure even contact between wax rims
– At this stage, the heals of acrylic basesmay touch, the interference may betrimmed but not to affect retention of bases
– Reduce lower occlusal rim so that the
VDO( between 2-dots) is 2-4 mm less
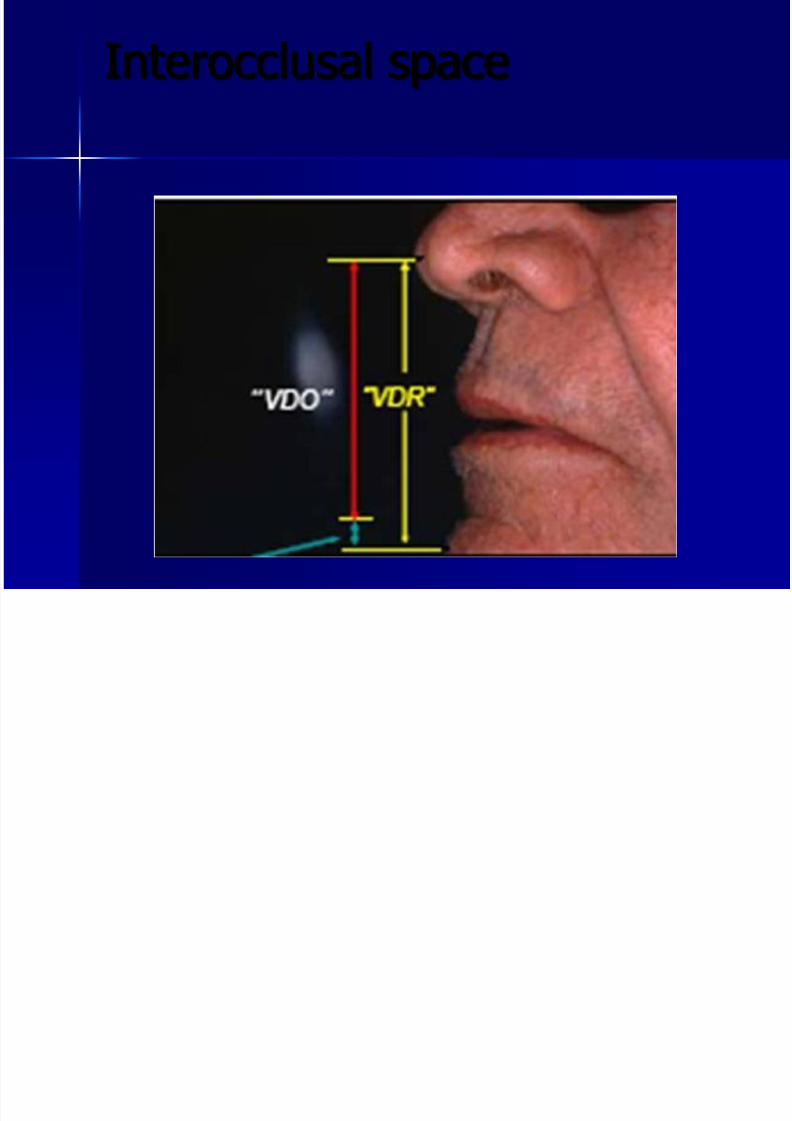
Interocclusal space
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 95/99
Interocclusal space
Jaw relations
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 96/99
Jaw relations
Arch form
– Posterior height of lower wax rim should
be 2/3 level up of retromolar pad – There should be 8-10mm from centre of
incisive papilla to labial surface of maxillary rim
Jaw relations

7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 97/99
Jaw relations
Record horizontal jaw relations
Retruded contact position: jaw
relationships in the horizontal plane atwhich the location of the occlusal rimswill be registered
Jaw relations
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 98/99
Jaw relations
Record horizontal jaw relations
– when the condyles are in most retruded
position in the fossa and the jaw musclesare relaxed, the mandible can be movedin a simple hinge like manner and the jawmust be in most retruded position
– Swallowing and closure – Tip of the tongue against posterior border
of upper base plate
Jaw relations
7/28/2019 Dr Ziad
http://slidepdf.com/reader/full/dr-ziad 99/99
Jaw relations
Measure Occlusal verticaldimension (VDO):
– This space is interocclusal spaceexisting between upper and lowerteeth when mandible in physiologicrest position